

Surgeon administered direct adductor canal block is as good as ultrasound guided adductor canal block in pain management in knee replacements- A retrospective case-control study
- PMID: 35514532
- PMCID: PMC9062125
- DOI: 10.1016/j.jor.2022.04.009
Surgeon administered direct adductor canal block is as good as ultrasound guided adductor canal block in pain management in knee replacements- A retrospective case-control study
Abstract
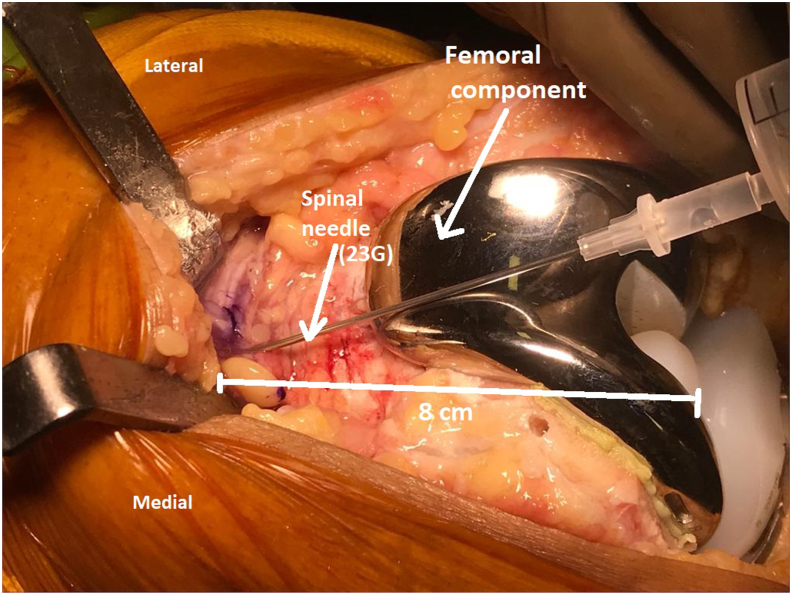
Aim: The aim of this study is to assess the feasibility of the DACB in a clinical setting and compare the efficacy of postoperative pain relief after TKR in the patients administered DACB versus USG guided ACB. Also to see efficacy and safety of USACB in patients operated with medial parapatellar and subvastus approach.
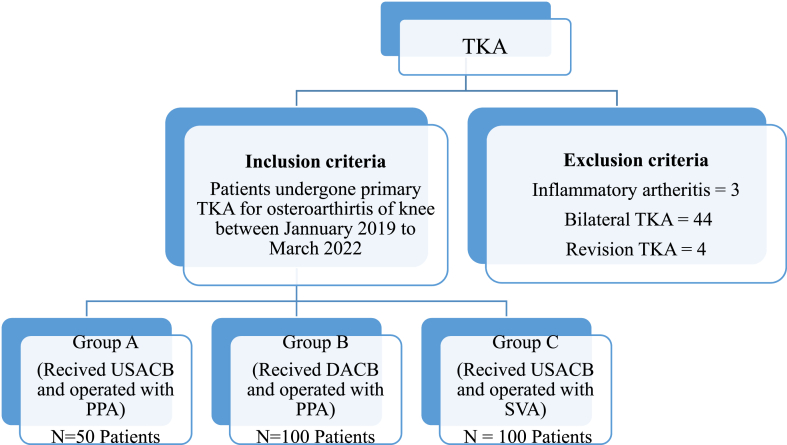
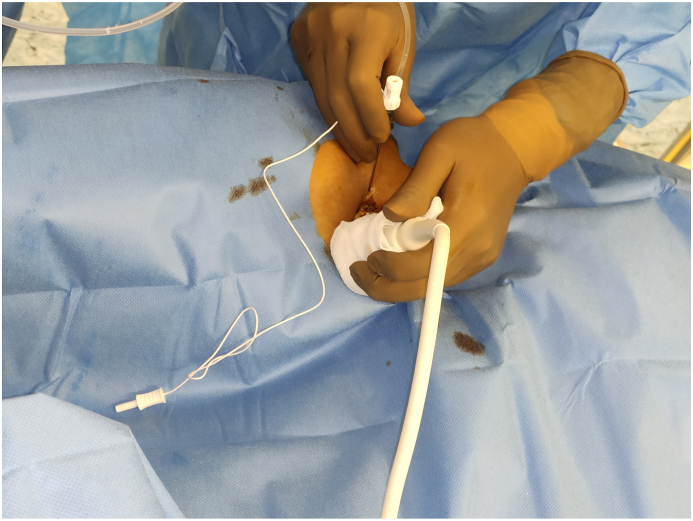
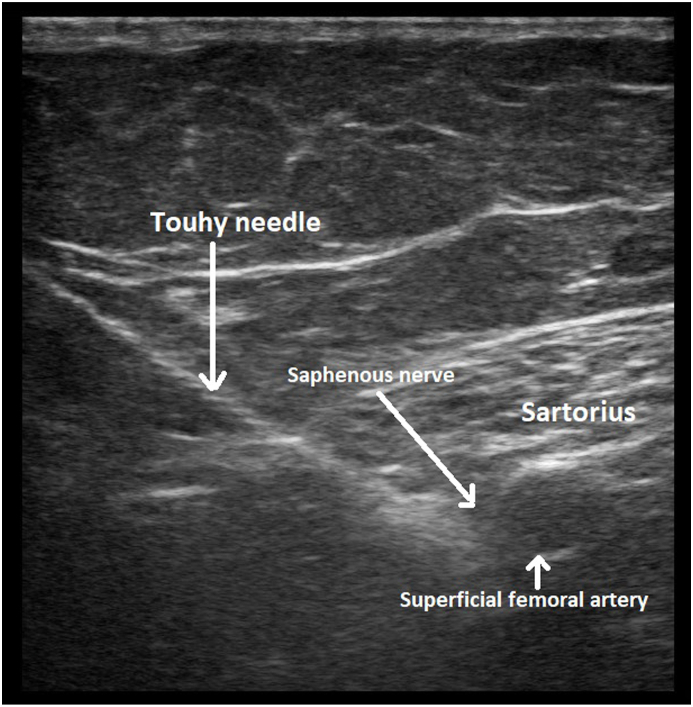
Material and methods: 250 consecutive patients operated with TKR between Jan 2019 to March 2022 were included. Group A included patients operated with medial parapatellar approach and received USACB, Group B included patients operated with medial parapatellar approach and received DACB while Group C included patients operated with subvastus approach and received USACB. VAS scores between three groups were compared at 12 and 24 h. All three groups of patients were otherwise treated identically in the hospital.
Results: The mean age and BMI was not statistically significant between the three groups. The mean VAS pain score at rest at 12 h was 3.06 ± 1.49 (Group A) vs 1.58 ± 1.19 (Group B) [p < 0.0001] and 3.06 ± 1.49 (Group A) vs 1.88 ± 1.18 (Group C) [p < 0.0001]; and at 24 h was 1.88 ± 1.31 (Group A) vs 2.39 ± 1.27 (Group B) [p = 0.023] and 1.88 ± 1.31 (Group A) vs 2.19 ± 1.29 (Group C) [p = 0.16]. The mean theatre time was 151.9 ± 11.37 min (Group A) vs 141.02 ± 19.46 min (Group B) (p = 0.0003) and 151.9 ± 11.37 min (Group A) vs 150.4 ± 28.74 min (Group C) (p = 0.72). Hospital stay was 3.82 ± 0.80 (Group A) vs 4.0 ± 1.09 (Group B) [p = 0.30] and 3.82 ± 0.80 (Group A) vs 2.7 ± 0.69 (Group C) [p < 0.0001]. Group B and Group C had one complication each.
Conclusion: USG ACB irrespective of approach used remains the gold standard in providing consistent pain relief and thereby facilitating early discharge. However, increased operating room turnover time and repeated top-ups remain a disadvantage. Both the quantum of pain relief and the potential downsides remained the same irrespective of the surgical approach used and whether or not steroid was added to the cocktail used for infiltration. On the other hand, DACB provides a short lasting (24 h) adequate pain relief after TKR with similar low complication rates. The technique of DACB may have a potential for a wider use especially in centres where outpatient arthroplasties are performed, if newer longer acting anaesthetic/analgesic combinations are devised.
Keywords: Direct adductor canal block; Pain assessment; Surgical time; Total knee replacement; USG guided Adductor canal block.
© 2022 Professor P K Surendran Memorial Education Foundation. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
None.
Figures
References
-
- Zhao X.Q., Jiang N., Yuan F.F., Wang L., Yu B. The comparison of adductor canal block with femoral nerve block following total knee arthroplasty: a systematic review with meta-analysis. J Anaesth. 2016 Oct 1;30(5):745–754. - PubMed
-
- YaDeau J.T., Cahill J.B., Zawadsky M.W., et al. The effects of femoral nerve blockade in conjunction with epidural analgesia after total knee arthroplasty. Anesth Analg. 2005 Sep 1;101(3):891–895. - PubMed
-
- Berend M.E., Berend K.R., Lombardi A.V., Jr. Advances in pain management: game changers in knee arthroplasty. Bone Joint Journal. 2014 Nov;96(11_Supple_A):7–9. - PubMed
-
- Wheeler M., Oderda G.M., Ashburn M.A., Lipman A.G. Adverse events associated with postoperative opioid analgesia: a systematic review. J Pain. 2002 Jun 1;3(3):159–180. - PubMed
LinkOut - more resources
Full Text Sources
