

Concomitant Hemophagocytic Lymphohistiocytosis and Cytomegalovirus Disease: A Case Based Systemic Review
- PMID: 35514747
- PMCID: PMC9063453
- DOI: 10.3389/fmed.2022.819465
Concomitant Hemophagocytic Lymphohistiocytosis and Cytomegalovirus Disease: A Case Based Systemic Review
Abstract
Background: Hemophagocytic lymphohistiocytosis (HLH) is an immune mediated life-threatening condition. It is driven by an overactivation of the immune system and causes inflammatory tissue damage potentially leading to organ failure and death. Primary HLH is caused by genetic mutations, while secondary HLH is triggered by external factors. Viral infections are a well-known cause of secondary HLH. Cytomegalovirus (CMV) is a virus in the herpes family known to cause HLH in rare cases.
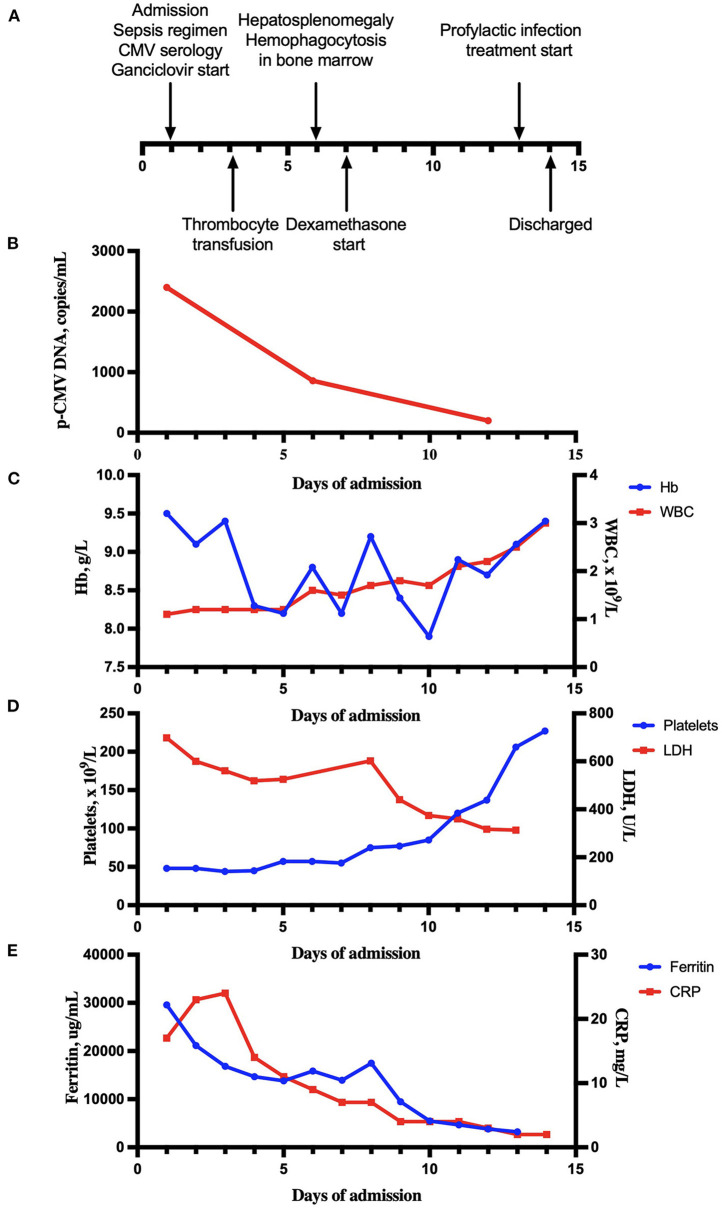
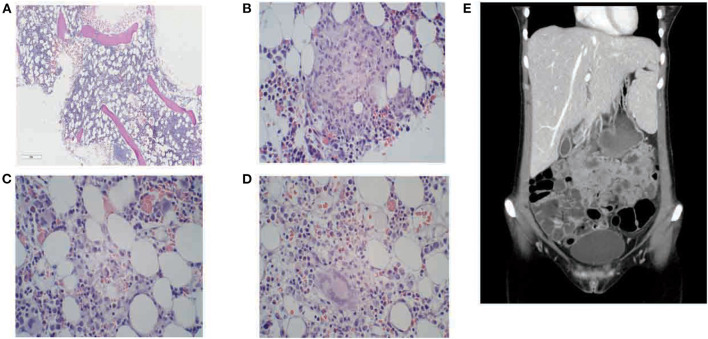
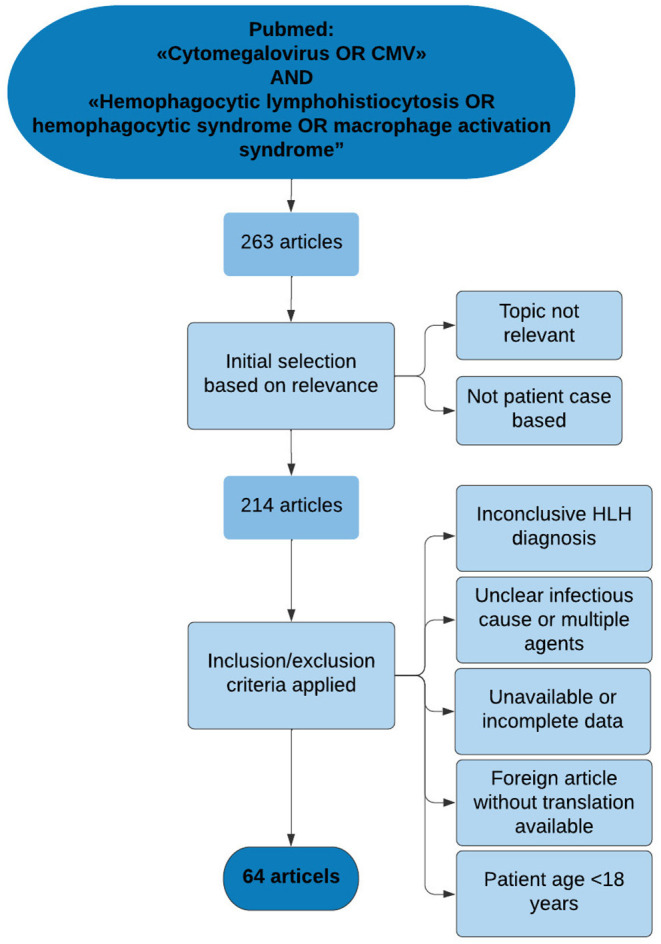
Methods: We report a recent case of CMV-induced HLH, followed by a systematic review of described cases of this rare disease entity, through a structured search in the medical database PubMed. All articles were assessed on a predetermined set of inclusion criteria.
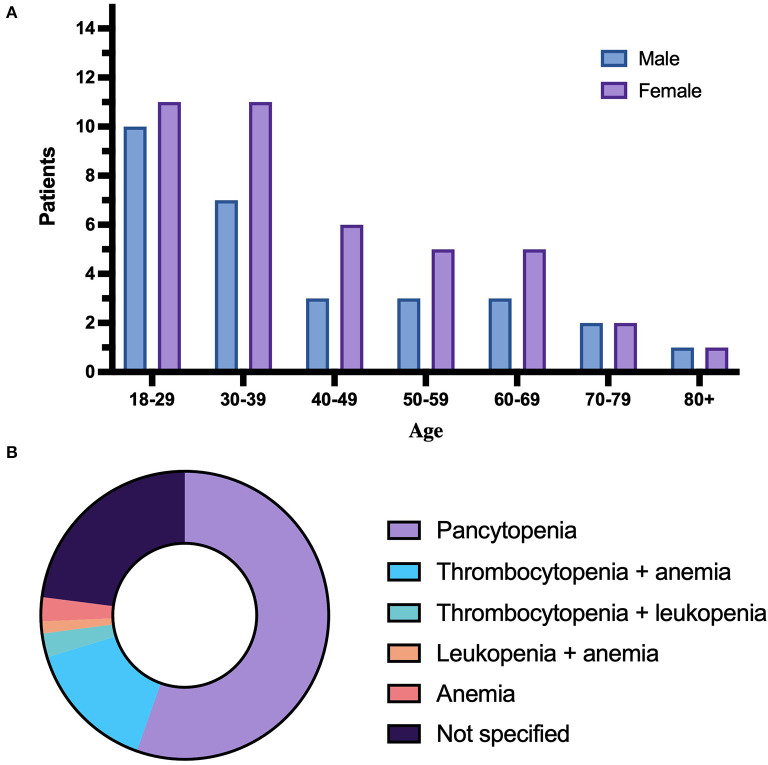
Results: A total of 74 patients (age > 18 years) with CMV-related HLH were identified, 29 men, 42 women, and three patients with unspecified gender. Median age was 37.5 years (range 18-80). Sixty-six patients (88%) had one or more comorbid conditions and 22 patients (30%) had inflammatory bowel disease (IBD), the most frequent comorbidity. Forty patients (54%) received some form of immunomodulating treatment prior to HLH development. The general treatment approach was in general dual, consisting of antiviral treatment and specific immunomodulating HLH treatment approaches. Treatment outcome was at 77% survival, while 23% had fatal outcome.
Conclusion: The findings highlight the importance of early diagnostic work up and treatment intervention. Ability to recognize the characteristic clinical traits and perform specific HLH diagnostic workup are key factors to ensure targeted diagnostic work and treatment intervention for this patient group.
Keywords: HLH; cytokines; cytomegalovirus (CMV); immunosuppression; inflammatory bowel diseases (IBD).
Copyright © 2022 Rolsdorph, Mosevoll, Helgeland and Reikvam.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Henter JI, Elinder G, Ost A. Diagnostic guidelines for hemophagocytic lymphohistiocytosis. The FHL Study Group of the Histiocyte Society. Semin Oncol. (1991) 18:29–33. - PubMed
Publication types
LinkOut - more resources
Full Text Sources