

Delphi consensus recommendation for optimization of pulmonary hypertension therapy focusing on switching from a phosphodiesterase 5 inhibitor to riociguat
- PMID: 35514769
- PMCID: PMC9063960
- DOI: 10.1002/pul2.12055
Delphi consensus recommendation for optimization of pulmonary hypertension therapy focusing on switching from a phosphodiesterase 5 inhibitor to riociguat
Abstract
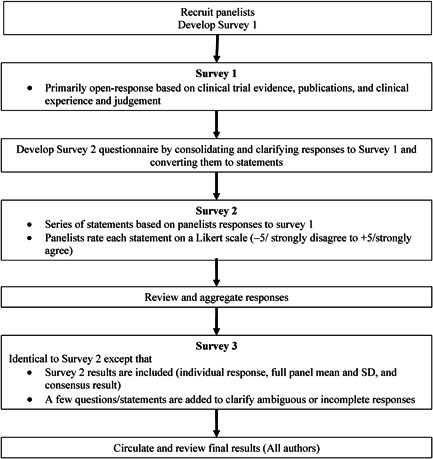
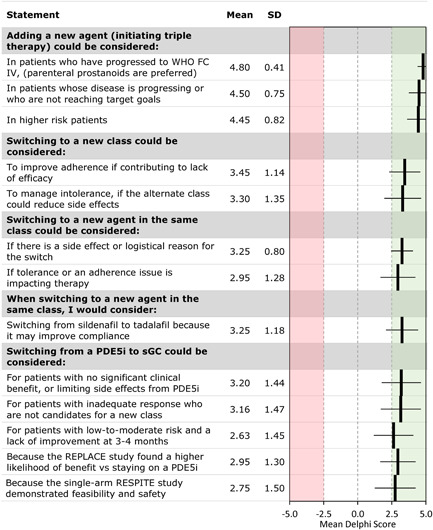
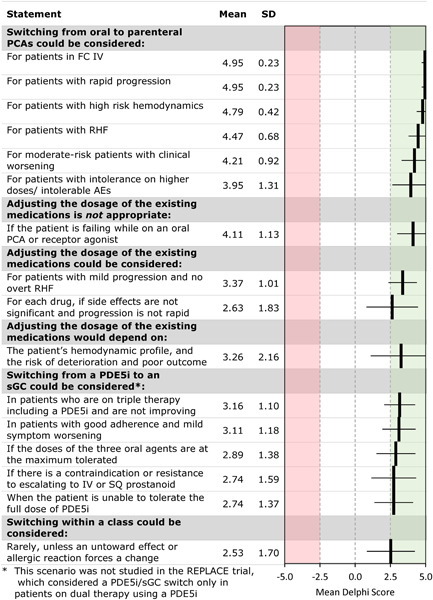
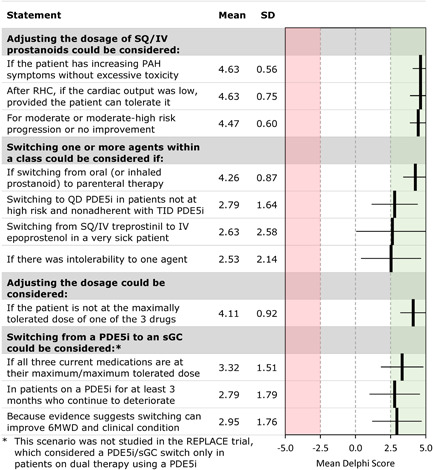
Dual combination therapy with a phosphodiesterase-5 inhibitor (PDE5i) and endothelin receptor antagonist is recommended for most patients with intermediate-risk pulmonary arterial hypertension (PAH). The RESPITE and REPLACE studies suggest that switching from a PDE5i to a soluble guanylate cyclase (sGC) activator may provide clinical improvement in this situation. The optimal approach to escalation or transition of therapy in this or other scenarios is not well defined. We developed an expert consensus statement on the transition to sGC and other treatment escalations and transitions in PAH using a modified Delphi process. The Delphi process used a panel of 20 physicians with expertise in PAH. Panelists answered three questionnaires on the management of treatment escalations and transitions in PAH. The initial questionnaire included open-ended questions. Later questionnaires consolidated the responses into statements that panelists rated on a Likert scale from -5 (strongly disagree) to +5 (strongly agree) to determine consensus. The Delphi process produced several consensus recommendations. Escalation should be considered for patients who are at high risk or not achieving treatment goals, by adding an agent from a new class, switching from oral to parenteral prostacyclins, or increasing the dose. Switching to a new class or within a class should be considered if tolerability or other considerations unrelated to efficacy are affecting adherence. Switching from a PDE5i to an SGC activator may benefit patients with intermediate risk who are not improving on their present therapy. These consensus-based recommendations may be helpful to clinicians and beneficial for patients when evidence-based guidance is unavailable.
Keywords: adherence; goal directed; tolerability; treat to target; treatment escalation.
© 2022 The Authors. Pulmonary Circulation published by John Wiley & Sons Ltd on behalf of Pulmonary Vascular Research Institute.
Conflict of interest statement
Franck F. Rahaghi reports consultation, research, and speakership honoraria from Bayer and Janssen, consultation and speakership from United Therapeutics, and consultation fees from Acceleron. Vijay P. Balasubramanian reports a research grant from United Therapeutics and serves on a speakers bureau for Bayer. Robert C. Bourge reports research grant support to my institution from United Therapeutics and Bayer, and service on a Scientific Advisory Board at United Therapeutics. Murali M. Chakinala reports grants or contracts from Actelion/Janssen, Bayer, Medtronic, NIH, Reata, Liquidia, Phase Bio, Complexa, United Therapeutics, Altavant, Trio Health Analytics, Reata, Acceleron, Arena, and Gossamer; consulting fees from Altavant, Vaderis Therapeutics, Aerovate, Reata, VWave, and Arena; honoraria from Bayer, Gilead, Simply Speaking, WebMD, and United Therapeutics; support for attending meetings and/or travel from Actelion/Janssen, United Therapeutics, Bayer, Acceleron, Reata, and Gilead; participation on a Data Safety Monitoring Board or Advisory Board for Actelion/Janssen, Express Scripts, Phase Bio, Altavant, Gossamer, United Therapeutics, Bayer, Acceleron, and Liquidia; and leadership or a fiduciary role in the Pulmonary Hypertension Association and the Cure HHT Global Research and Medical Advisory Board. Michael S. Eggert reports research contracts with United Therapeutics (BREEZE and ADVANCE Outcomes), Acceleron, and Actelion. Jean M. Elwing reports grants from Actelion, Acceleron, Reata, United Therapeutics, Liquidia, Phase Bio, Complexa, Gossamer Bio, Bayer, Arena, Eiger, Akros, Bellerophon, and Lung LLC and consulting fees from United Therapeutics, Acceleron, Liquidia, Altavant, Bayer, Gossamer Bio, Actelion, Bayer. Jeremy Feldman reports consulting and giving talks for Bayer, United Therapeutics, and Jansen. Christopher King reports personal fees from Actelion, personal fees from Genentech, United Therapeutics, and Boehringer Ingelheim; has served on advisory boards for and is on the Speakers’ Bureau of Actelion, Boehringer‐Ingelheim Pharmaceuticals, and United Therapeutics. James R. Klinger reports that his institution receives research funding from United Technologies, service on a Steering Committee and a Clinical Outcomes Committee for Bayer, and a leadership role in the Pulmonary Hypertension Association. Stephen C. Mathai reports personal fees from United Therapeutics; participation on a data safety monitoring board or advisory board from United Therapeutics, Actelion, and Bayer, and leadership or a fiduciary role in the PCORI Rare Disease Advisory Panel and the World Symposium on Pulmonary Hypertension. John Wesley McConnell reports consulting fees from Actelion, Bayer, Gossamer, Altavant, and Liquidia; honoraria from Actelion, Bayer, Simply Speaking, Impact PH, and Reata, and participation on a data safety monitoring board or advisory board for Actelion, Liquidia, Gossamer, and Altavant. Harold I. Palevsky reports honoraria for serving on scientific advisory boards for Acceleron, Actelion/Janssen, PhaseBio and United Therapeutics, and serving on a DSMB for United Therapeutics. Ricardo Restrepo‐Jaramillo reports serving on speaker's bureau for United Therapeutics, Bayer, and Actelion. Zeenat Safdar reports serving on a speakers bureau, consultation and advisory boards for Actelion, United Therapeutics, Boehringer Ingelheim, Bayer, and Roche. Jeffrey S. Sager reports personal fees from Bayer pharmaceuticals, grants and personal fees from United Therapeutics, grants and personal fees from Janssen (J and J), and grants from Reata outside the submitted work. Namita Sood reports a speaking fee from Bayer. Roxana Sulica reports research grants from Bayer, United Therapeutics, Complexa, and Reata, and serves on advisory boards for Actelion, Bayer, United Therapeutics, and Reata. R. James White reports research grants from United Therapeutics, Reata, Bayer, Merck, and Janssen and consulting fees from Merck and Bayer. Nicholas S. Hill reports honoraria from Axon Research for this study; grants to his institution from Actelion, Bayer, Gilead, and United Therapeutics; consulting fees from United Therapeutics; and participation in Data Safety Monitoring Boards for United Therapeutics and Pfizer. All authors had access to the Delphi questionnaire analysis and data and participated in the review, revision, and approval of the content of the manuscript for submission. Charles D. Burger reports no disclosures or conflicts of interest.
Figures
References
-
- Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, Ghofrani A, Gomez Sanchez MA, Hansmann G, Klepetko W, Lancellotti P, Matucci M, McDonagh T, Pierard LA, Trindade PT, Zompatori M, Hoeper M. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J. 2015. Oct;46(4):903–75. 10.1183/13993003.01032-2015 - DOI - PubMed
-
- Hoeper MM, Simonneau G, Corris PA, Ghofrani HA, Klinger JR, Langleben D, Naeije R, Jansa P, Rosenkranz S, Scelsi L, Grunig E, Vizza CD, Chang M, Colorado P, Meier C, Busse D, Benza RL. RESPITE: switching to riociguat in pulmonary arterial hypertension patients with inadequate response to phosphodiesterase‐5 inhibitors. Eur Respir J. 2017. Sep;50(3):1602425. 10.1183/13993003.02425-2016 - DOI - PMC - PubMed
-
- Hoeper MM, Al‐Hiti H, Benza RL, Chang SA, Corris PA, Gibbs JSR, Grunig E, Jansa P, Klinger JR, Langleben D, McLaughlin VV, Meyer GMB, Ota‐Arakaki J, Peacock AJ, Pulido T, Rosenkranz S, Vizza CD, Vonk‐Noordegraaf A, White RJ, Chang M, Kleinjung F, Meier C, Paraschin K, Ghofrani HA, Simonneau G, Olschewski H, Delcroix M, Andrade‐Lima M, de Amorim Correac R, Figueiredo Campos F, Ota Arakaki J, Meyer G, De Souza R, Langleben D, Al‐Hiti H, Jansa P, Mellemkjær S, Bauer F, Montani D, Simonneau G, Dromann D, Ghofrani HA, Grunig E, Halank M, Held M, Hoeper M, Klose H, Kneidinger N, Leuchte H, Opitz C, Rosenkranz S, Wilkens H, Wirtz H, Karvounis H, Pitsiou G, Orfanos S, D'Alto M, Ghio S, Vizza C, Vitulo P, Nakayama T, Maki H, Tatebe S, de los Rios Ibarra M, Pulido T, Van Dijk A, Vonk‐Noordegraaf A, Roleder T, Castro G, Loureiro M, Robalo‐Martins S, Barbera J, Lazaro M, Perez‐Penate G, Roman A, Cheng CC, Hsu CH, Hsu HH, Atahan E, Mogulkoc Bishop N, Okumus N, Onen Z, Chang HJ, Chang SA, Lee JS, Kim HK, Coghlan J, Corris P, Church A, Condliffe R, Gibbs J, Peacock A, Wort S, Allen R, Allen S, Awdish R, Benza R, DeSouza S, Feldman J, Johri S, Klinger J, Layish D, McConnell J, McLaughlin V, Migliore C, Rahaghi F, Rischard F, Robbins I, Satterwhite L, Shah T, Sulica R, White R. Switching to riociguat versus maintenance therapy with phosphodiesterase‐5 inhibitors in patients with pulmonary arterial hypertension (REPLACE): a multicentre, open‐label, randomised controlled trial. Lancet Respir Med. 2021. Jun;9(6):573–84. 10.1016/s2213-2600(20)30532-4 - DOI - PubMed
