

Multilayered macular hemorrhages as an unusual complication of transorbital neuroendoscopic surgery
- PMID: 35514795
- PMCID: PMC9062224
- DOI: 10.1016/j.ajoc.2022.101556
Multilayered macular hemorrhages as an unusual complication of transorbital neuroendoscopic surgery
Abstract
Purpose: To report a case of multilayered intraocular hemorrhage at the posterior pole as a complication of transorbital neuroendoscopic surgery.
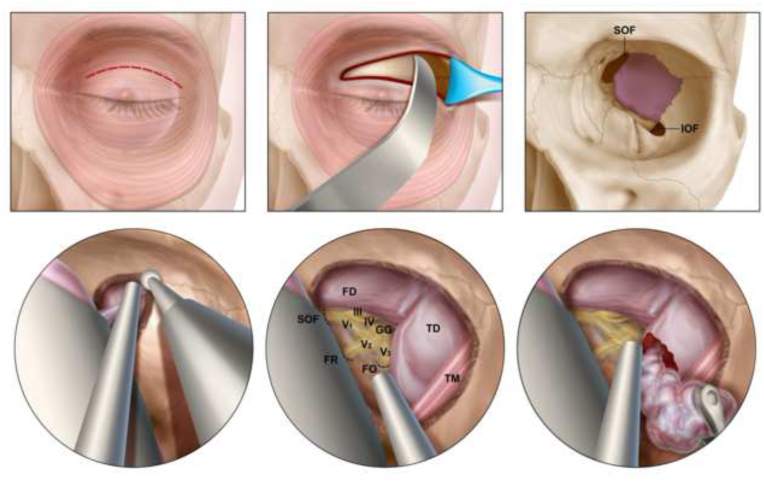
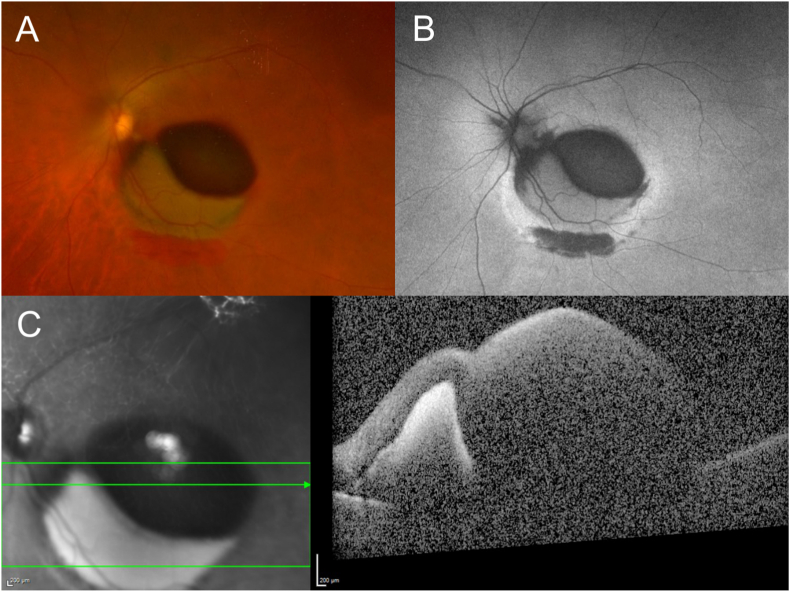
Observations: Our patient underwent an uncomplicated endoscopic transorbital resection of a left sphenoid wing meningioma. In the immediate post-operative period, the patient reported blurred vision of her left eye, and dilated fundus examination demonstrated multilayered hemorrhages at the posterior pole. No intracranial hemorrhage was identified on post-operative imaging. Due to persistent subnormal visual acuity and non-clearing hemorrhage over several weeks of follow-up, a pars plana vitrectomy with peeling of the internal limiting membrane was performed to clear the hemorrhagic component obscuring the macula.
Conclusions and importance: We report the first case of multilayered intraocular hemorrhages at the posterior pole, mimicking Terson syndrome, in the absence of intracranial hemorrhage or elevated intracranial pressure as a complication of transorbital surgery.
Keywords: Meningioma; Neuroendoscopic; Spheno-orbital; Sphenoid wing; Surgery; Terson syndrome; Transorbital.
© 2022 The Authors.
Conflict of interest statement
The following authors have no financial disclosures: WF, VSN, BWB, MJD, FH, KJG, DJD, THS, AO.
Figures



References
-
- Fountas K.N., Kapsalaki E.Z., Lee G.P., et al. Terson hemorrhage in patients suffering aneurysmal subarachnoid hemorrhage: predisposing factors and prognostic significance. J Neurosurg. 2008;109(3):439–444. - PubMed
-
- Naseri A., Blumenkranz M.S., Horton J.C. Terson's syndrome following epidural saline injection. Neurology. 2001;57(2):364. - PubMed
-
- Pagani-Estévez G.L., Chen J.J., Watson J.C., Leavitt J.A. Acute vision loss secondary to epidural blood patch: Terson syndrome. Reg Anesth Pain Med. 2016;41(2):164–168. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
