

Rapid Disease Control in First-Line Therapy-Resistant Mucous Membrane Pemphigoid and Bullous Pemphigoid with Omalizumab as Add-On Therapy: A Case Series Of 13 Patients
- PMID: 35514989
- PMCID: PMC9065717
- DOI: 10.3389/fimmu.2022.874108
Rapid Disease Control in First-Line Therapy-Resistant Mucous Membrane Pemphigoid and Bullous Pemphigoid with Omalizumab as Add-On Therapy: A Case Series Of 13 Patients
Abstract
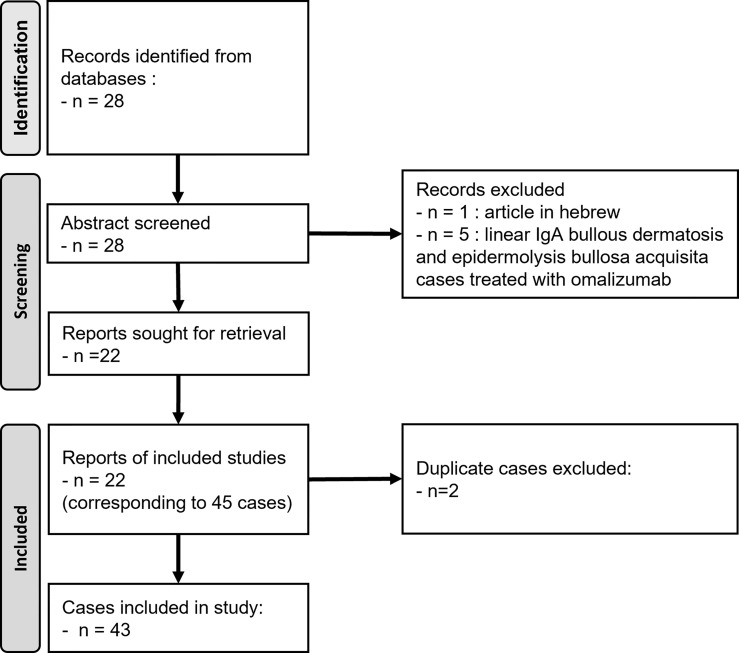
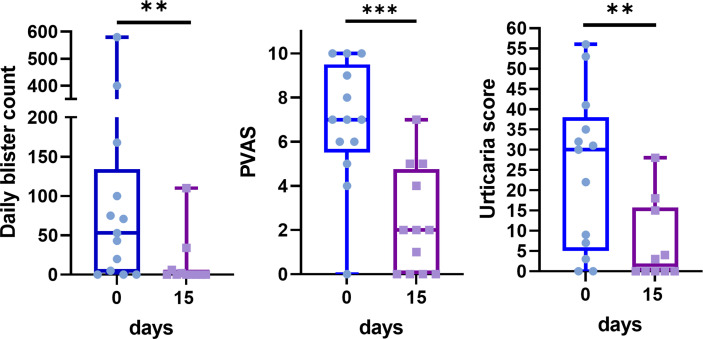
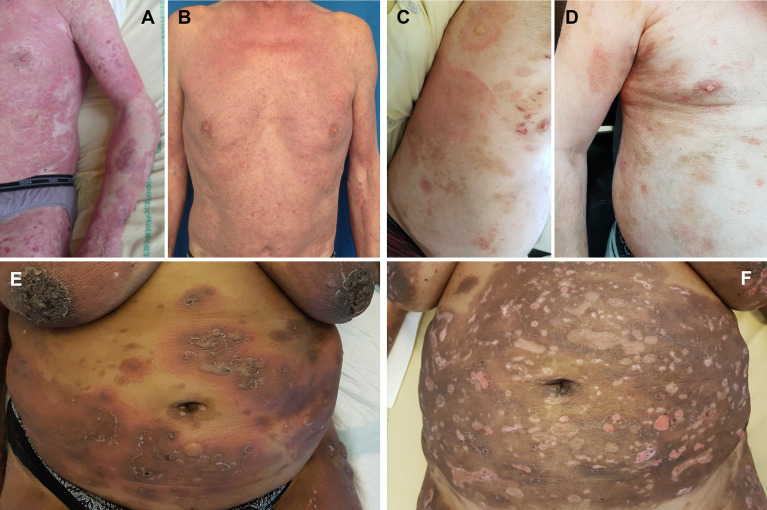
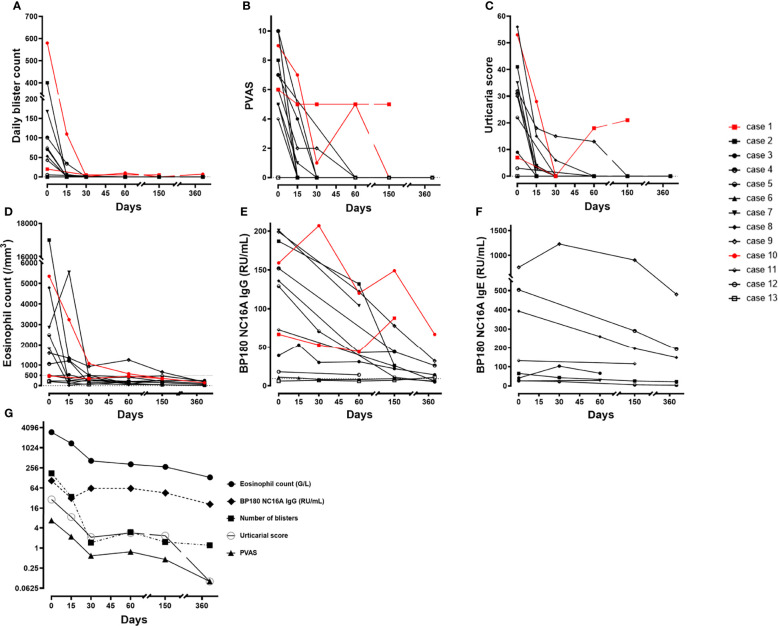
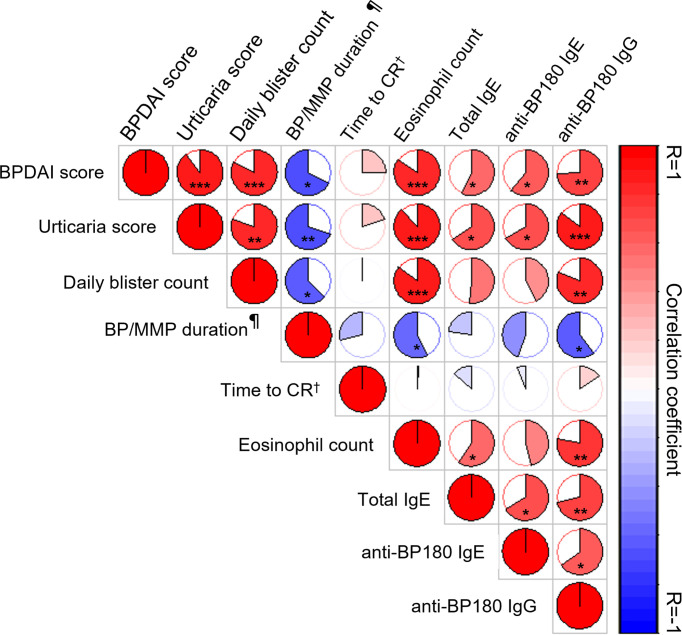
The role of IgE autoantibodies has been demonstrated in the pathogenesis of bullous pemphigoid for many years. Recently, omalizumab (OMZ), a humanized monoclonal anti-IgE antibody that depletes total serum IgE, has been used off-label in a few case series of bullous pemphigoids demonstrating a rapid efficacy and allowing significant improvements or complete remission as add-on therapy in first-line treatment-resistant patients. Herein, we report the largest retrospective study to evaluate OMZ effectiveness in patients with subepidermal autoimmune blistering diseases. Our series included 13 patients from a single center with bullous pemphigoid or mucous membrane pemphigoid, of whom 7 had mucous membrane involvement. OMZ was added to the unchanged immunosuppressive therapies. Detailed clinical and immunological data during the first year were collected, notably for specific anti-BP180-NC16A IgE and IgG, and the median total follow-up was 30 months (range: 3-81). Our series demonstrated that OMZ induced a significant improvement in pruritus, urticarial score, and daily blister count on day 15, allowing disease control to be achieved in a 1-month median time and complete remission (CR) in a 3-month median time in 85% of these patients previously in therapeutic impasse. At the end of the follow-up, 31% of patients achieved CR on minimal therapy after OMZ weaning without relapses, and 54% achieved CR on OMZ continuation with a minimal dose of concomitant treatment. Two patients experienced therapeutic failure (15%). At baseline, clinical variables reflecting activity were significantly positively correlated with eosinophil blood count, total IgE serum level, specific anti-BP180 IgE and IgG. While baseline anti-BP180 IgG and specific anti-BP180 IgE were significantly positively correlated, only the two patients who experienced a therapeutic failure with OMZ did not fit with this correlation, demonstrating elevated levels of anti-BP180 IgG with no measurable BP180-specific IgE. Follow-up of immunological variables demonstrated a rapid decrease of eosinophilia towards normalization, whereas a slower decline towards negativation was observed over 1 year for anti-BP180 IgG and anti BP180 IgE in patients who responded to OMZ. This case series demonstrated that OMZ is a rapidly effective biologic therapy for refractory bullous pemphigoid and mucous membrane pemphigoid, permitting rapid disease control and reduction of concomitant therapeutics.
Keywords: Anti-BP180 IgE; Anti-BP180 IgG; Immunoglobulin E (IgE); autoimmune bullous diseases (AIBDs); autoimmune skin diseases; bullous pemphigoid (BP); mucous membrane pemphigoid (MMP); omalizumab (Xolair).
Copyright © 2022 Alexandre, Bohelay, Gille, Le Roux-Villet, Soued, Morin, Caux, Grootenboer-Mignot and Prost-Squarcioni.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical