

Defining Discriminatory Antibody Fingerprints in Active and Latent Tuberculosis
- PMID: 35514994
- PMCID: PMC9066635
- DOI: 10.3389/fimmu.2022.856906
Defining Discriminatory Antibody Fingerprints in Active and Latent Tuberculosis
Erratum in
-
Corrigendum: Defining discriminatory antibody fingerprints in active and latent tuberculosis.Front Immunol. 2023 Nov 21;14:1329784. doi: 10.3389/fimmu.2023.1329784. eCollection 2023. Front Immunol. 2023. PMID: 38077391 Free PMC article.
Abstract
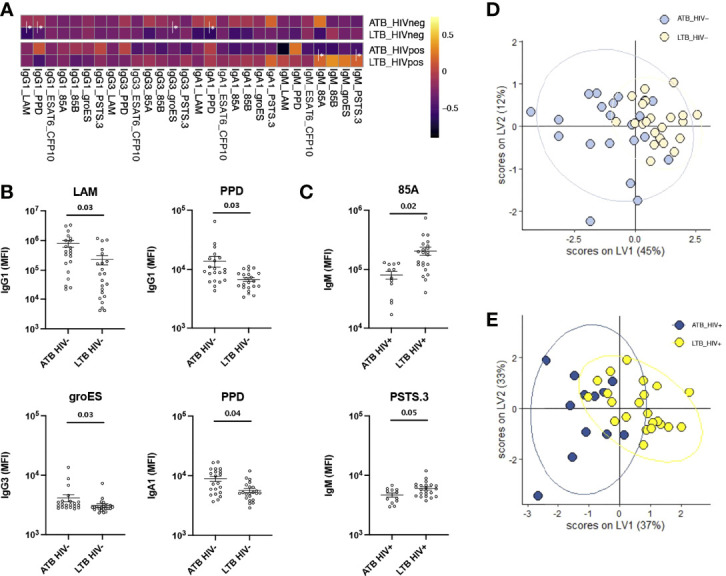
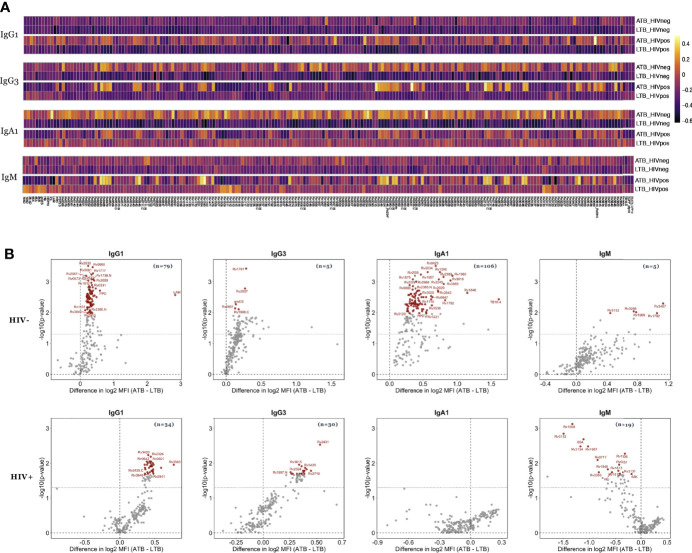
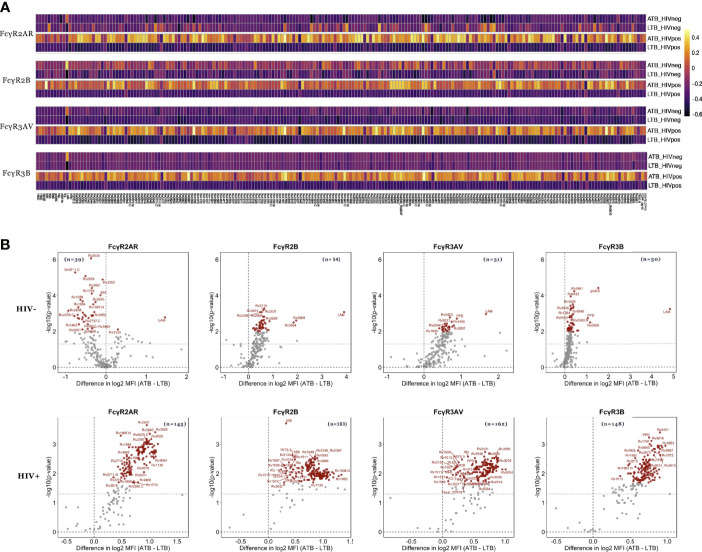
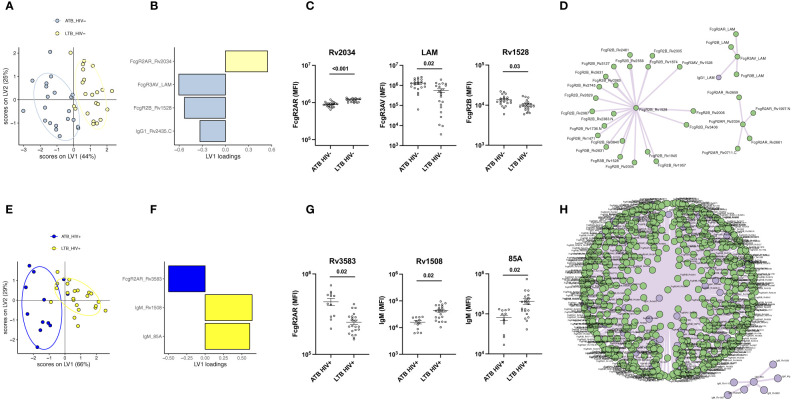
Tuberculosis (TB) is among the leading causes of death worldwide from a single infectious agent, second only to COVID-19 in 2020. TB is caused by infection with Mycobacterium tuberculosis (Mtb), that results either in a latent or active form of disease, the latter associated with Mtb spread. In the absence of an effective vaccine, epidemiologic modeling suggests that aggressive treatment of individuals with active TB (ATB) may curb spread. Yet, clinical discrimination between latent (LTB) and ATB remains a challenge. While antibodies are widely used to diagnose many infections, the utility of antibody-based tests to diagnose ATB has only regained significant traction recently. Specifically, recent interest in the humoral immune response to TB has pointed to potential differences in both targeted antigens and antibody features that can discriminate latent and active TB. Here we aimed to integrate these observations and broadly profile the humoral immune response across individuals with LTB or ATB, with and without HIV co-infection, to define the most discriminatory humoral properties and diagnose TB disease more easily. Using 209 Mtb antigens, striking differences in antigen-recognition were observed across latently and actively infected individuals that was modulated by HIV serostatus. However, ATB and LTB could be discriminated, irrespective of HIV-status, based on a combination of both antibody levels and Fc receptor-binding characteristics targeting both well characterized (like lipoarabinomannan, 38 kDa or antigen 85) but also novel Mtb antigens (including Rv1792, Rv1528, Rv2435C or Rv1508). These data reveal new Mtb-specific immunologic markers that can improve the classification of ATB versus LTB.
Keywords: HIV; active and latent tuberculosis; antibodies; biomarkers; diagnostics.
Copyright © 2022 Nziza, Cizmeci, Davies, Irvine, Jung, Fenderson, de Kock, Hanekom, Franken, Day, Ottenhoff and Alter.
Conflict of interest statement
GA is a founder and equity holder in Systems Seromyx and Leyden Labs. GA’s interests were reviewed and managed by MGH and Partners HealthCare in accordance with their conflict of interest policies. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical