

Lymphocyte to Monocyte Ratio and C-Reactive Protein Combination as the Best Simple Predictor of Treatment Response in Cirrhotic Patients with Culture Negative Neutrocytic Ascites
- PMID: 35515960
- PMCID: PMC9040302
- DOI: 10.14744/SEMB.2021.58219
Lymphocyte to Monocyte Ratio and C-Reactive Protein Combination as the Best Simple Predictor of Treatment Response in Cirrhotic Patients with Culture Negative Neutrocytic Ascites
Abstract
Objectives: The aim of this study was to evaluate the most ideal inflammatory markers for treatment response and to determine a cutoff value that could predict response to treatment for culture negative neutrocytic ascite (CNNA) patients.
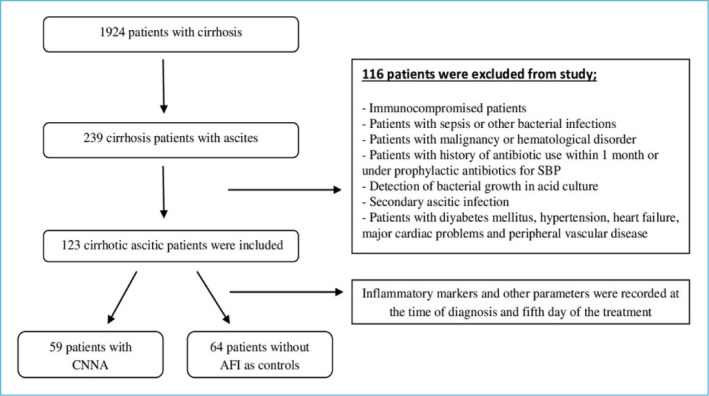
Methods: This is a retrospective cross-sectional case-controlled study. Patients with CNNA were evaluated by taking ascites fluid sampling at the beginning and on the 5th day of treatment. Neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), and neutrophil-to-monocyte ratio were calculated.
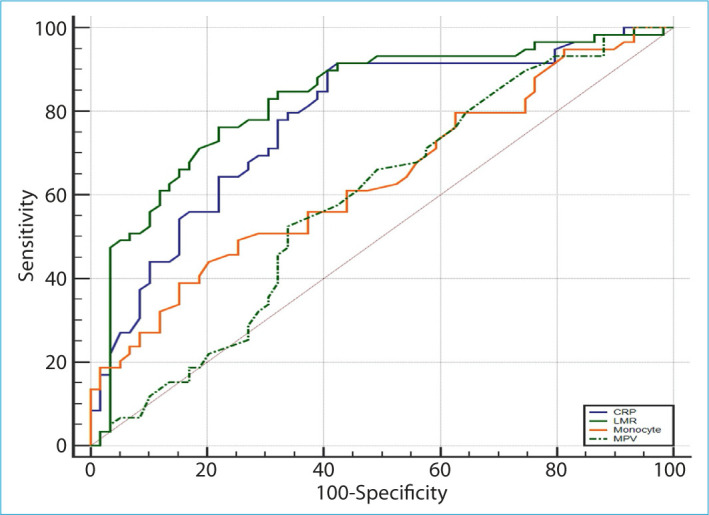
Results: Of the 123 cases with cirrhotic ascites disease, 59 were CCNA and 64 were the control group without ascite-fluid infection. There were statistically significant differences for blood monocyte count, NLR (p<0.01), LMR, and C-reactive protein (CRP) (p<0.001) between two groups. Patients in the CNNA group were compared before and after treatment among themselves for the treatment response. There was statistically significant difference in mean platelet volume, monocyte, LMR, and CRP (p<0.05) between two groups. After receiver operator characteristics curve analysis, the best cutoff value for monocyte was <0.64 × 103/μL (sensitivity 49.2%, specificity 74.6%, positive predictive value [PPV] 65.9%, and negative predictive value [NPV] 59.5%) (p<0.01), for LMR was ≥1.7 (sensitivity 76.3%, specificity 78%, PPV 77.6%, and NPV 76.7%), and for CRP was ≤18 mg/L (sensitivity 91.5% specificity 57.6%, PPV 68.4%, and NPV 87.2%) (p<0.001). When LMR and CRP were used together, sensitivity (86.5%), specificity (83.1%), PPV (83.6%), and NPV (86%) were found to be statistically significantly higher (p<0.001).
Conclusion: Our results showed that in cirrhotic patients with CNNA, combined LMR + CRP can be used as a novel, low cost and non-invasive test to predict treatment response.
Keywords: Ascitic fluid infection; c-reactive protein; cirrhosis; culture negative neutrocytic ascites; lymphocyte to monocyte ratio.
©Copyright 2022 by The Medical Bulletin of Sisli Etfal Hospital - Available online at www.sislietfaltip.org.
Figures
References
-
- Ginés P, Quintero E, Arroyo V, Terés J, Bruguera M, Rimola A, et al. Compensated cirrhosis: natural history and prognostic factors. Hepatology. 1987;7:122–8. - PubMed
-
- Ngamruengphong S, Nugent K, Rakvit A, Parupudi S. Potential preventability of spontaneous bacterial peritonitis. Dig Dis Sci. 2011;56:2728–34. - PubMed
-
- Arvaniti V, D'Amico G, Fede G, Manousou P, Tsochatzis E, Pleguezuelo M, et al. Infections in patients with cirrhosis increase mortality four-fold and should be used in determining prognosis. Gastroenterology. 2010;139:1246–56. - PubMed
-
- Fernández J, Gustot T. Management of bacterial infections in cirrhosis. J Hepatol. 2012;56(Suppl 1):S1–12. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous