

Where Are We Heading With Fluid Responsiveness and Septic Shock?
- PMID: 35518529
- PMCID: PMC9065654
- DOI: 10.7759/cureus.23795
Where Are We Heading With Fluid Responsiveness and Septic Shock?
Abstract
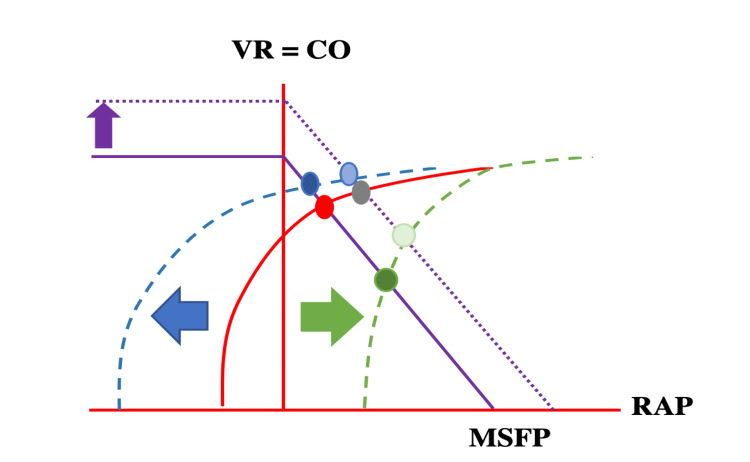
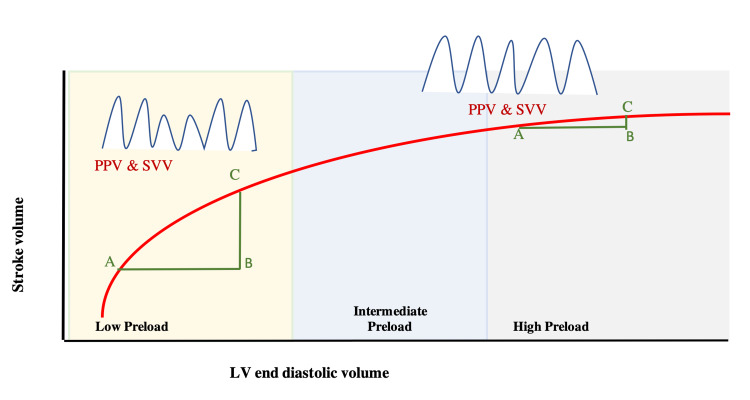
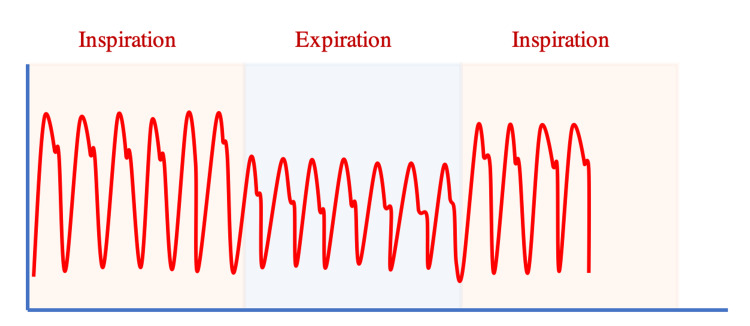
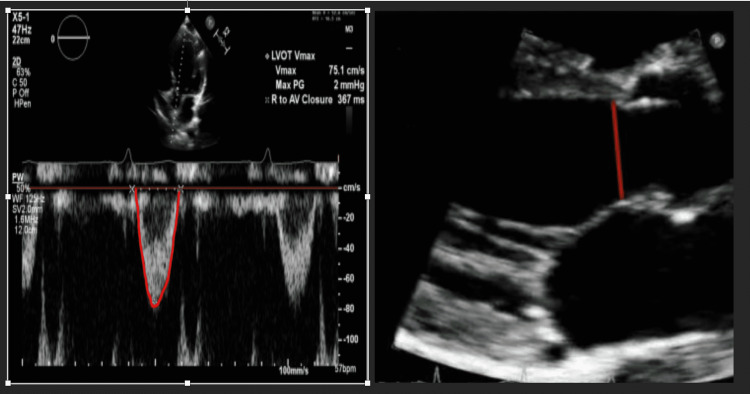
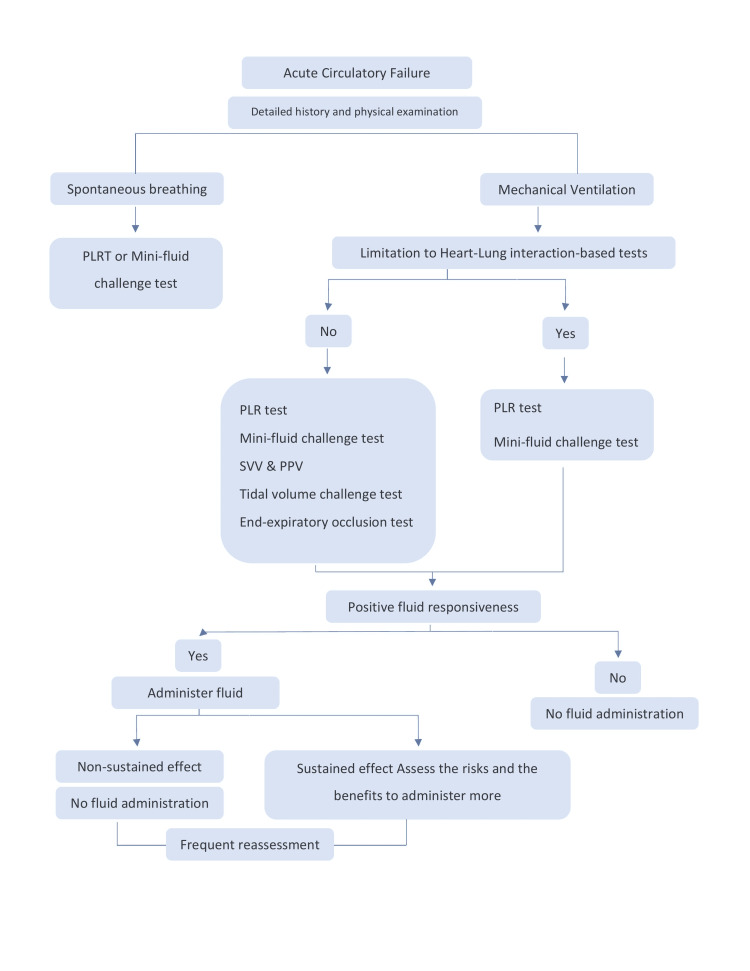
When hypovolemia is left uncorrected, it can lead to poor tissue oxygenation and organ dysfunction. On the other hand, excessive fluid administration can increase the risk of complications. Assessing volume responsiveness in critically ill patients is therefore crucial. In this article we summarized the literature addressing the most sensitive and specific dynamic predictors for fluid responsiveness, to help clarify the best way to guide clinicians in managing patients with shock. Data were collected from PubMed and EMBASE of high-quality articles, randomized controlled trials (RCTs), retrospective research, and metanalyses; articles were identified from January 2000 to February 2021. We identified and critically reviewed the published peer-reviewed literature investigating the dynamic predictors to assess fluid responsiveness. Evidence suggests that the traditional use of static predictors for fluid responsiveness should be abandoned. Over the last 20 years, a number of dynamic tests have been developed. These tests are based on the principle of inducing short-term changes in cardiac preload using heart-lung interactions. However, in routine practice the conditions to meet the requirements of these dynamic parameters are frequently not met. Therefore, more dynamic predictors that do not depend on heart-lung interaction have developed such as the mini fluid challenge test and passive leg raising test These tests have fewer limitations and higher sensitivity and specificity compared to the other tests.
Keywords: fluid responsiveness; liberal vs restricted approach to fluid resuscitation in septic shock; passive leg raising; pocus; pulse pressure variation.
Copyright © 2022, Megri et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Predicting fluid responsiveness in ICU patients: a critical analysis of the evidence. Michard F, Teboul JL. Chest. 2002;121:2000–2008. - PubMed
-
- Fluid resuscitation in septic shock: a positive fluid balance and elevated central venous pressure are associated with increased mortality. Boyd JH, Forbes J, Nakada TA, Walley KR, Russell JA. Crit Care Med. 2011;39:259–265. - PubMed
-
- Comparison of two fluid-management strategies in acute lung injury. Wiedemann HP, Wheeler AP, Bernard GR, et al. N Engl J Med. 2006;354:2564–2575. - PubMed
-
- Basic concepts of heart-lung interactions during mechanical ventilation. Grübler MR, Wigger O, Berger D, Blöchlinger S. Swiss Med Wkly. 2017;147:0. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous