

Analysis of a pitfall in congenital adrenal hyperplasia newborn screening: evidence of maternal use of corticoids detected on dried blood spot
- PMID: 35521805
- PMCID: PMC9254290
- DOI: 10.1530/EC-22-0101
Analysis of a pitfall in congenital adrenal hyperplasia newborn screening: evidence of maternal use of corticoids detected on dried blood spot
Abstract
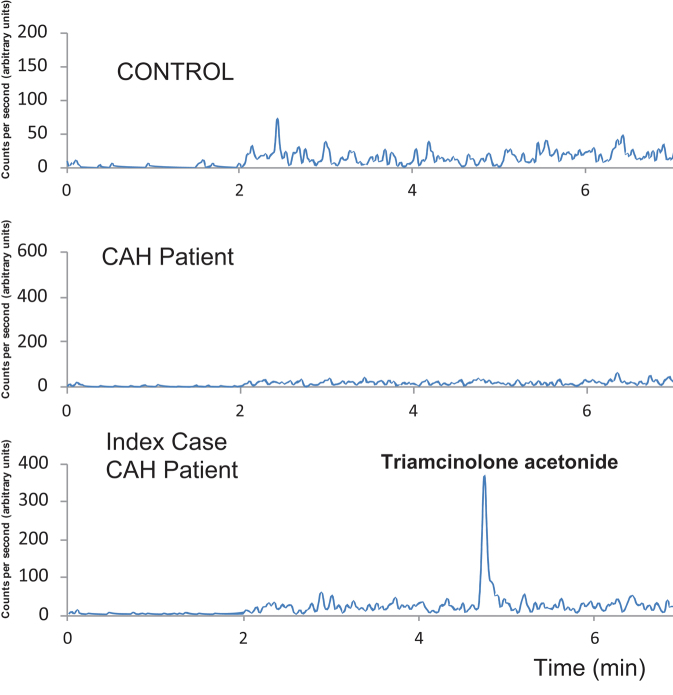
Neonatal screening for congenital adrenal hyperplasia (CAH) faces many specific challenges. It must be done using a performant analytical approach that combines sensitivity and specificity to capture the potential causes of mortality during the first week of life, such as salt wasting and glucocorticoid deficiency. Here, we confirm that maternal inhaled corticosteroid intake during pregnancy is a possible cause of missed CAH diagnosis. Thanks to liquid chromatography coupled with tandem mass spectrometry (LC-MS/MS) analysis, we were able to quantify endogenous steroid metabolites and also detect the presence of exogenous steroids in the dried blood spot of a newborn. Adding LC-MS/MS analysis as second-tier test, especially one that includes both 17-hydroxyprogesterone and 21-deoxycortisol measurements, would probably improve CAH diagnosis. In familial neonatal screening one could also look for maternal corticosteroid therapies that are hidden to prevent false-negative tests.
Keywords: 17-hydroxyprogesterone; CAH; dried blood spot; glucocorticoid treatment; newborn screening.
Figures
References
-
- Hannon WH.Clinical, Laboratory Standards I. Blood Collection on Filter Paper for Newborn Screening Programs. Wayne, PA, USA: Approved Standard. Clinical and Laboratory Standards; Institute, 2013.
-
- Lacey JM, Minutti CZ, Magera MJ, Tauscher AL, Casetta B, McCann M, Lymp J, Hahn SH, Rinaldo P, Matern D. Improved specificity of newborn screening for congenital adrenal hyperplasia by second-tier steroid profiling using tandem mass spectrometry. Clinical Chemistry 200450621–625. ( 10.1373/clinchem.2003.027193) - DOI - PubMed
-
- Janzen N, Peter M, Sander S, Steuerwald U, Terhardt M, Holtkamp U, Sander J. Newborn screening for congenital adrenal hyperplasia: additional steroid profile using liquid chromatography-tandem mass spectrometry. Journal of Clinical Endocrinology and Metabolism 2007922581–2589. ( 10.1210/jc.2006-2890) - DOI - PubMed
LinkOut - more resources
Full Text Sources
