

Predictors of metformin monotherapy failure in gestational diabetes mellitus
- PMID: 35521811
- PMCID: PMC9175587
- DOI: 10.1530/EC-21-0540
Predictors of metformin monotherapy failure in gestational diabetes mellitus
Abstract
Objective: Metformin has emerged as a safe and effective pharmacological alternative to insulin in gestational diabetes mellitus (GDM), being associated with lower maternal weight gain and hypoglycemia risk. Nevertheless, glycemic control is unaccomplished in a considerable proportion of women only treated with metformin. We aim to determine the metformin monotherapy failure rate in GDM and to identify predictors of its occurrence.
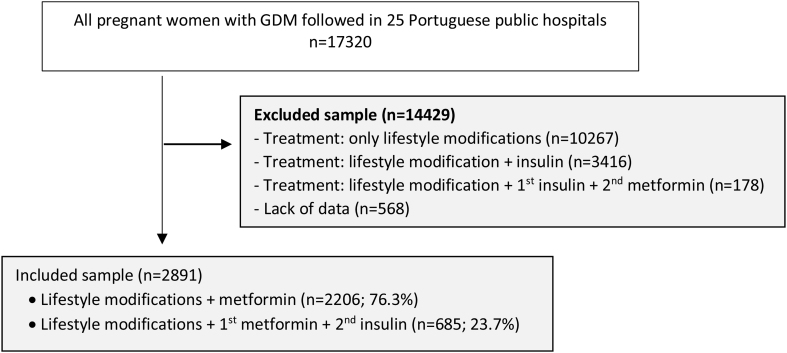
Design and methods: This was a retrospective multicenter study including pregnant women with GDM patients who started metformin as a first-line pharmacological treatment (n = 2891). A comparative analysis of clinical and analytical data between the group of women treated with metformin monotherapy and those needing combined therapy with insulin was performed.
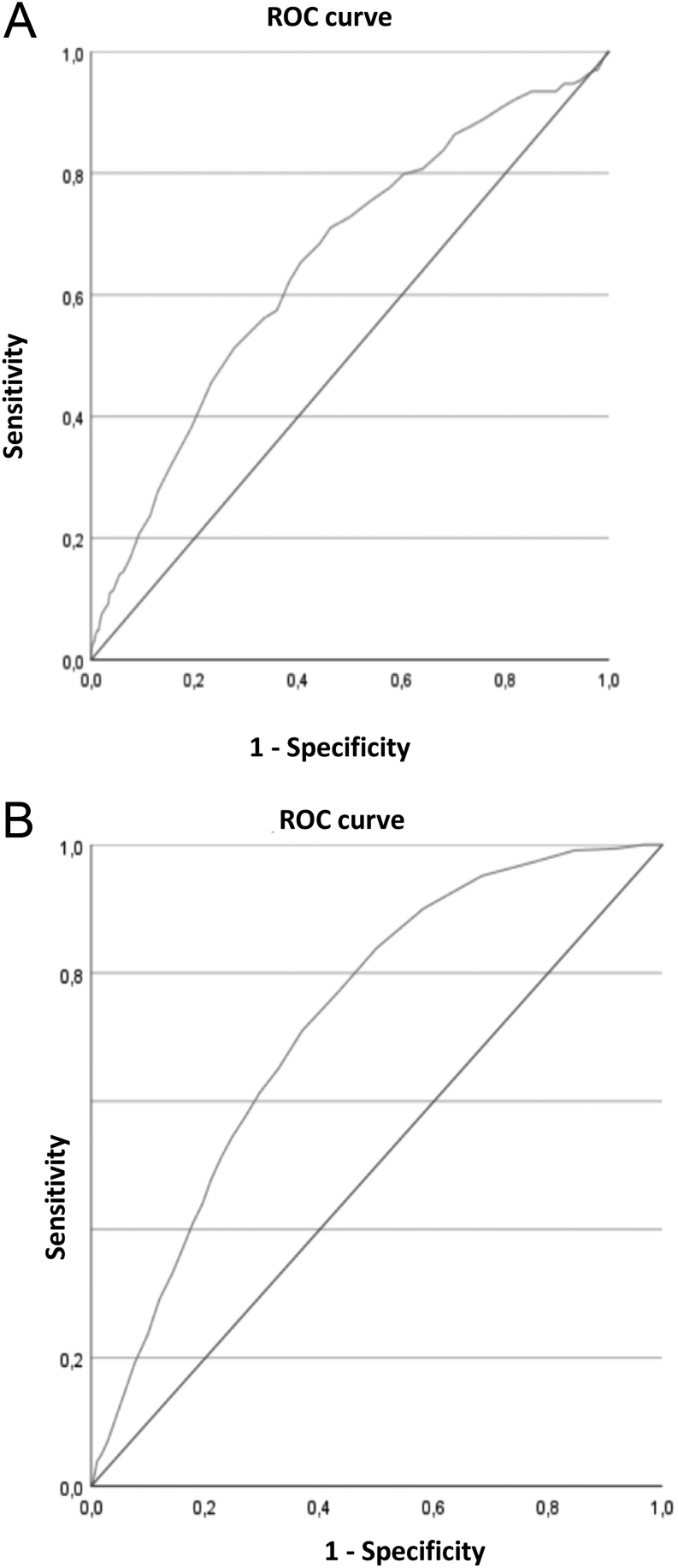
Results: In 685 (23.7%) women with GDM, combined therapy to achieve adequate glycemic control was required. Higher pregestational BMI (OR 1.039; CI 95% 1.008-1.071; P-value = 0.013), higher fasting plasma glucose (PG) levels in oral glucose tolerance test (OGTT) (OR 1.047; CI 95% 1.028-1.066; P-value <0.001) and an earlier gestational age (GA) at metformin introduction (0.839; CI 95% 0.796-0.885, P-value < 0.001) were independent predictive factors for metformin monotherapy failure. The best predictive cutoff values were a fasting PG in OGTT ≥87 mg/dL and GA at metformin introduction ≤29 weeks.
Conclusions: In 685 (23.7%) women, combined therapy with insulin to reach glycemic control was required. Higher pre-gestational BMI, fasting PG levels in OGTT ≥87 mg/dL and introduction of metformin ≤29 weeks of GA were independent predictive factors for metformin monotherapy failure. The early recognition of these characteristics can contribute to the establishment of individualized therapeutic strategies and attain better metabolic control during pregnancy.
Keywords: OGTT; diagnosis; failure; insulin; metformin; monotherapy; treatment; women.
Figures
Similar articles
-
Predictors of metformin failure in gestational diabetes mellitus (GDM).Diabetes Metab Syndr. 2018 May;12(3):405-410. doi: 10.1016/j.dsx.2018.01.003. Epub 2018 Jan 31. Diabetes Metab Syndr. 2018. PMID: 29576523
-
Identification of metformin poor responders, requiring supplemental insulin, during randomization of metformin versus insulin for the control of gestational diabetes mellitus.J Obstet Gynaecol Res. 2016 Jun;42(6):640-7. doi: 10.1111/jog.12950. Epub 2016 Mar 15. J Obstet Gynaecol Res. 2016. PMID: 26992090 Clinical Trial.
-
Report of the Committee on the classification and diagnostic criteria of diabetes mellitus.Diabetes Res Clin Pract. 2002 Jan;55(1):65-85. doi: 10.1016/s0168-8227(01)00365-5. Diabetes Res Clin Pract. 2002. PMID: 11755481
-
[Gestational diabetes mellitus (Update 2019)].Wien Klin Wochenschr. 2019 May;131(Suppl 1):91-102. doi: 10.1007/s00508-018-1419-8. Wien Klin Wochenschr. 2019. PMID: 30980150 Review. German.
-
[Gestational Diabetes Mellitus].Vnitr Lek. 2016 Fall;62(11 Suppl 4):S52-61. Vnitr Lek. 2016. PMID: 27921426 Review. Czech.
References
-
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel, Metzger BE, Gabbe SG, Persson B, Buchanan TA, Catalano PA, Damm P, Dyer AR, Leiva A, Hod M, Kitzmiler JLet al.International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 201033676–682. - PMC - PubMed
-
- Raposo JF.Diabetes: factos e números – 2016, 2017 e 2018. Revista Portuguesa de Diabetes 20201519–27.
LinkOut - more resources
Full Text Sources
