

Th1, Th2, and Th17 cells are dysregulated, but only Th17 cells relate to C-reactive protein, D-dimer, and mortality risk in Stanford type A aortic dissection patients
- PMID: 35522124
- PMCID: PMC9169215
- DOI: 10.1002/jcla.24469
Th1, Th2, and Th17 cells are dysregulated, but only Th17 cells relate to C-reactive protein, D-dimer, and mortality risk in Stanford type A aortic dissection patients
Abstract
Background: T helper (Th) cells are closely involved in vascular inflammation, endothelial dysfunction, and atherogenesis, which are the hallmarks of aortic dissection (AD). This study aimed to evaluate the clinical value of Th1, Th2, and Th17 cell measurements in Stanford type A AD patients.
Methods: Stanford type A AD patients (N=80) and non-AD patients with chest pain (N = 40) were recruited. Then, Th1, Th2, and Th17 cells in peripheral blood CD4+ T cells from all participants were detected by flow cytometry. The 30-day mortality of Stanford type A AD patients was recorded.
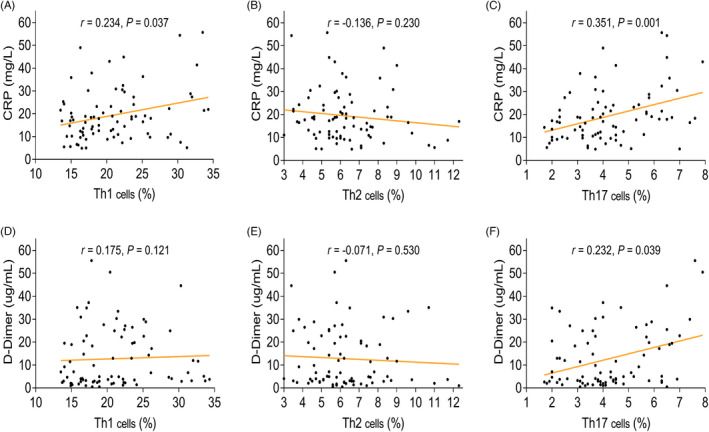
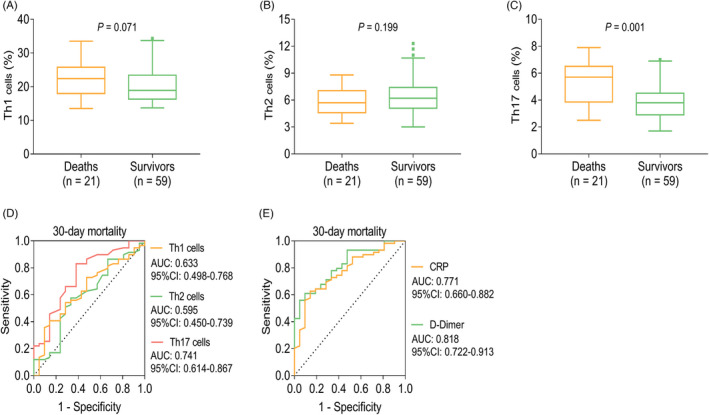
Results: Th1 and Th17 cells were higher, while Th2 cells were lower in Stanford type A AD patients compared with non-AD patients (all p < 0.001). Meanwhile, Th1 cells (area under curve (AUC): 0.734, 95% confidence interval (CI): 0.640-0.828), Th2 cells (AUC: 0.841, 95% CI: 0.756-0.925), and Th17 cells (AUC: 0.898, 95% CI: 0.839-0.957) could distinguish Stanford type A patients from non-AD patients. Moreover, Th1 cells (p = 0.037) and Th17 cells (p = 0.001) were positively related to CRP, and Th17 cells (p = 0.039) were also positively associated with D-dimer in Stanford type A AD patients. Furthermore, Th17 cells were elevated in deaths compared with survivors (p = 0.001), also, it could estimate 30-day mortality risk in Stanford type A AD patients with an AUC of 0.741 (95% CI: 0.614-0.867), which was similar to the value of CRP (AUC: 0.771, 95% CI: 0.660-0.882), but lower than the value of D-dimer (AUC: 0.818, 95% CI: 0.722-0.913).
Conclusion: Th1, Th2, and Th17 cells are dysregulated, but only the Th17 cells relate to CRP, D-dimer, and 30-day mortality risk in Stanford type A AD patients.
Keywords: C-reactive protein; D-dimer; 30-day mortality risk; T helper cells; stanford type A aortic dissection.
© 2022 The Authors. Journal of Clinical Laboratory Analysis published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
-
- Juraszek A, Czerny M, Rylski B. Update in aortic dissection. Trends Cardiovasc Med. 2021;15:200‐213. - PubMed
-
- Sherk WM, Khaja MS, Williams DM. Anatomy, pathology, and classification of aortic dissection. Tech Vasc Interv Radiol. 2021;24(2):100746. - PubMed
-
- Jassar AS, Sundt TM 3rd. How should we manage type A aortic dissection? Gen Thorac Cardiovasc Surg. 2019;67(1):137‐145. - PubMed
MeSH terms
Substances
Grants and funding
- H2015055/Natural Science Foundation of Heilongjiang Science and Technology Department
- 20-205-4-016/Research on Synergistic Innovation of Vital Signs Signal Collection and Transmission and Intelligent Processing in Emergency Medical Evacuation
- 20QNPY090/Research on Monitoring System of Vital Signs Based on Air Transport and Wear for Critical Patients in Battlefield
- 81900369/National Natural Science Foundation of China
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
