

Interobserver Variability in CT-based Morphologic Tumor Response Assessment of Colorectal Liver Metastases
- PMID: 35522139
- PMCID: PMC9152692
- DOI: 10.1148/rycan.210105
Interobserver Variability in CT-based Morphologic Tumor Response Assessment of Colorectal Liver Metastases
Abstract
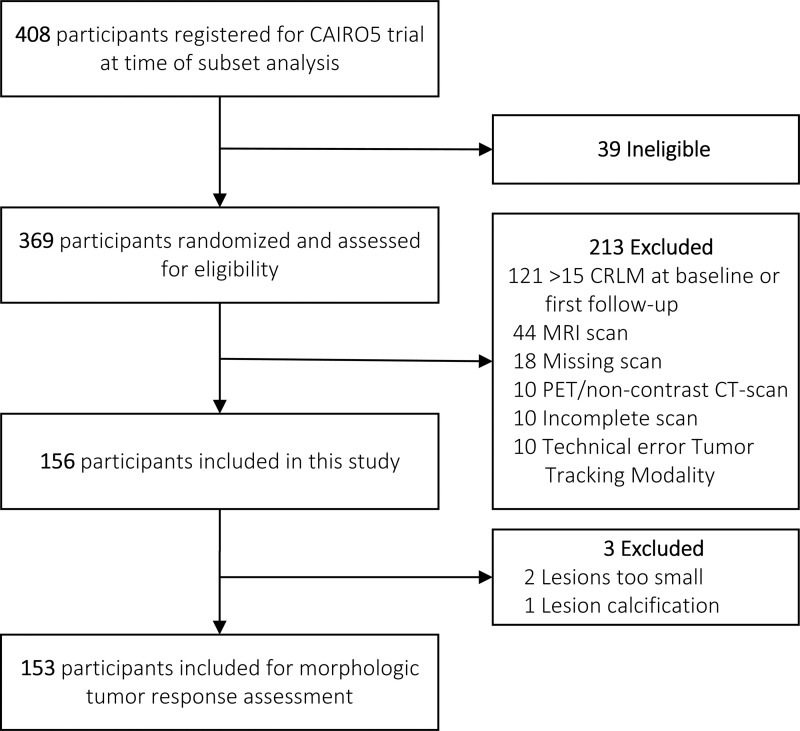
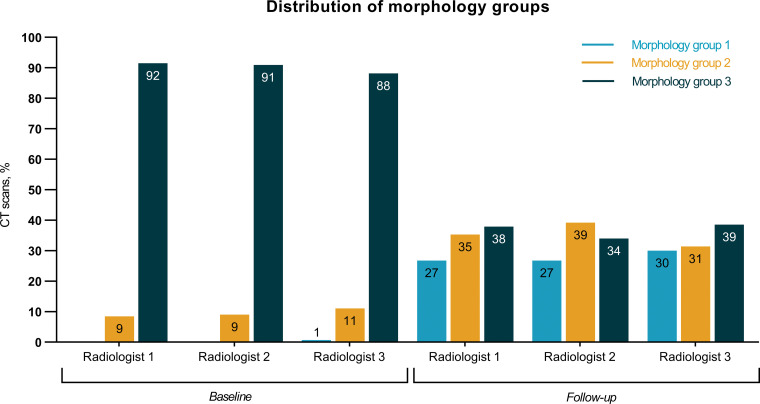
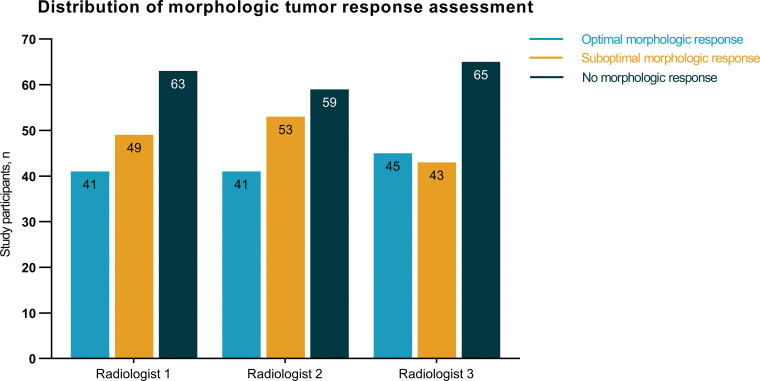
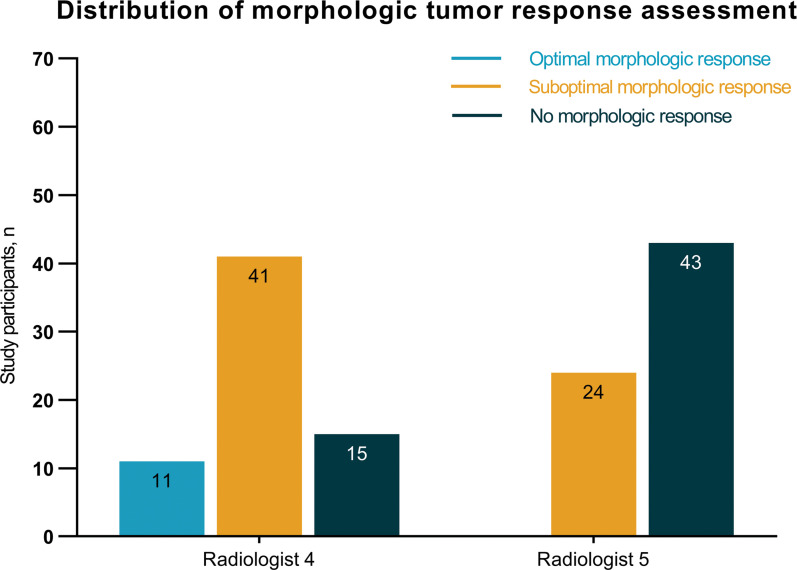
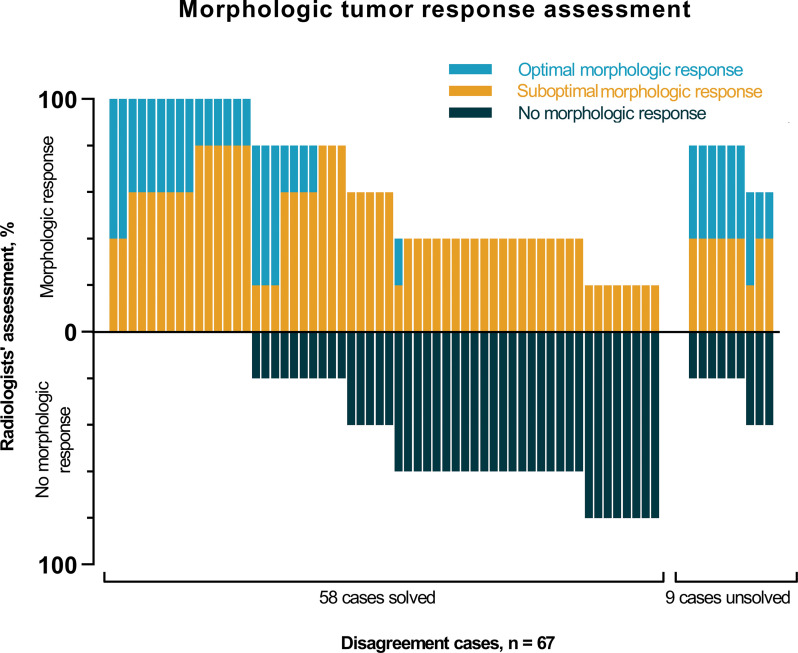
Purpose To evaluate interobserver variability in the morphologic tumor response assessment of colorectal liver metastases (CRLM) managed with systemic therapy and to assess the relation of morphologic response with gene mutation status, targeted therapy, and Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 measurements. Materials and Methods Participants with initially unresectable CRLM receiving different systemic therapy regimens from the randomized, controlled CAIRO5 trial (NCT02162563) were included in this prospective imaging study. Three radiologists independently assessed morphologic tumor response on baseline and first follow-up CT scans according to previously published criteria. Two additional radiologists evaluated disagreement cases. Interobserver agreement was calculated by using Fleiss κ. On the basis of the majority of individual radiologic assessments, the final morphologic tumor response was determined. Finally, the relation of morphologic tumor response and clinical prognostic parameters was assessed. Results In total, 153 participants (median age, 63 years [IQR, 56-71]; 101 men) with 306 CT scans comprising 2192 CRLM were included. Morphologic assessment performed by the three radiologists yielded 86 (56%) agreement cases and 67 (44%) disagreement cases (including four major disagreement cases). Overall interobserver agreement between the panel radiologists on morphology groups and morphologic response categories was moderate (κ = 0.53, 95% CI: 0.48, 0.58 and κ = 0.54, 95% CI: 0.47, 0.60). Optimal morphologic response was particularly observed in patients treated with bevacizumab (P = .001) and in patients with RAS/BRAF mutation (P = .04). No evidence of a relationship between RECIST 1.1 and morphologic response was found (P = .61). Conclusion Morphologic tumor response assessment following systemic therapy in participants with CRLM demonstrated considerable interobserver variability. Keywords: Tumor Response, Observer Performance, CT, Liver, Metastases, Oncology, Abdomen/Gastrointestinal Clinical trial registration no. NCT02162563 Supplemental material is available for this article. © RSNA, 2022.
Keywords: Abdomen/Gastrointestinal; CT; Liver; Metastases; Observer Performance; Oncology; Tumor Response.
Conflict of interest statement
Figures
References
-
- Siegel RL , Miller KD , Jemal A . Cancer statistics, 2019 . CA Cancer J Clin 2019. ; 69 ( 1 ): 7 – 34 . - PubMed
-
- Elferink MAG , de Jong KP , Klaase JM , Siemerink EJ , de Wilt JHW . Metachronous metastases from colorectal cancer: a population-based study in North-East Netherlands . Int J Colorectal Dis 2015. ; 30 ( 2 ): 205 – 212 . - PubMed
-
- van der Geest LGM , Lam-Boer J , Koopman M , Verhoef C , Elferink MA , de Wilt JH . Nationwide trends in incidence, treatment and survival of colorectal cancer patients with synchronous metastases . Clin Exp Metastasis 2015. ; 32 ( 5 ): 457 – 465 . - PubMed
-
- de Ridder JAM , van der Stok EP , Mekenkamp LJ , et al. . Management of liver metastases in colorectal cancer patients: a retrospective case-control study of systemic therapy versus liver resection . Eur J Cancer 2016. ; 59 ( 13 ): 21 . - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
