

Long-Term Outcomes of the Excluded Rectum in Crohn's Disease: A Multicenter International Study
- PMID: 35522225
- PMCID: PMC10210615
- DOI: 10.1093/ibd/izac099
Long-Term Outcomes of the Excluded Rectum in Crohn's Disease: A Multicenter International Study
Abstract
Background: Many patients with Crohn's disease (CD) require fecal diversion. To understand the long-term outcomes, we performed a multicenter review of the experience with retained excluded rectums.
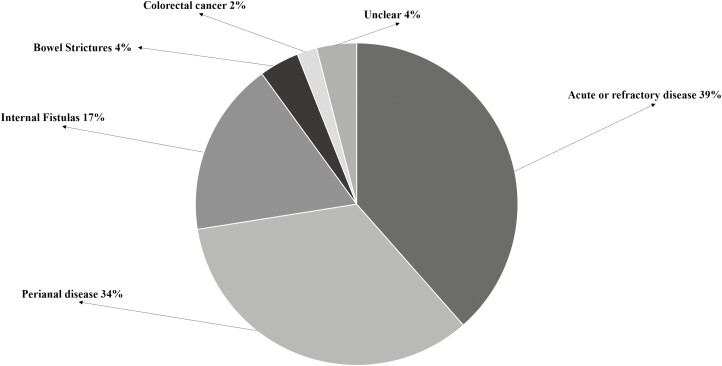
Methods: We reviewed the medical records of all CD patients between 1990 and 2014 who had undergone diversionary surgery with retention of the excluded rectum for at least 6 months and who had at least 2 years of postoperative follow-up.
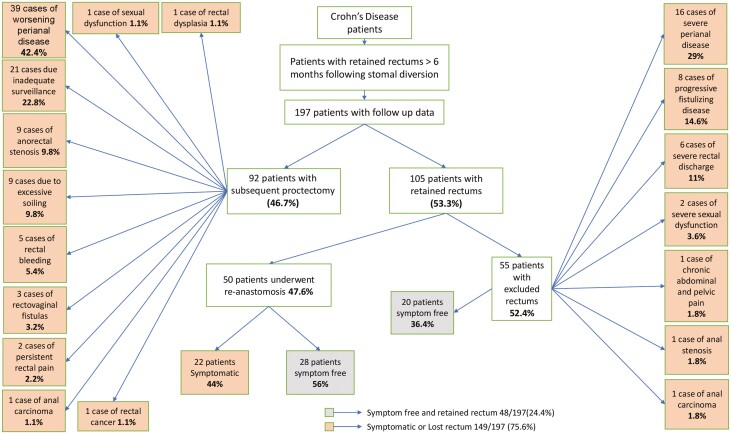
Results: From all the CD patients in the institutions' databases, there were 197 who met all our inclusion criteria. A total of 92 (46.7%) of 197 patients ultimately underwent subsequent proctectomy, while 105 (53.3%) still had retained rectums at time of last follow-up. Among these 105 patients with retained rectums, 50 (47.6%) underwent reanastomosis, while the other 55 (52.4%) retained excluded rectums. Of these 55 patients whose rectums remained excluded, 20 (36.4%) were symptom-free, but the other 35 (63.6%) were symptomatic. Among the 50 patients who had been reconnected, 28 (56%) were symptom-free, while 22(44%) were symptomatic. From our entire cohort of 197 cases, 149 (75.6%) either ultimately lost their rectums or remained symptomatic with retained rectums, while only 28 (14.2%) of 197, and only 4 (5.9%) of 66 with initial perianal disease, were able to achieve reanastomosis without further problems. Four patients developed anorectal dysplasia or cancer.
Conclusions: In this multicenter cohort of patients with CD who had fecal diversion, fewer than 15%, and only 6% with perianal disease, achieved reanastomosis without experiencing disease persistence.
Keywords: Crohn’s Disease; Perianal disease; Rectum; Surgery.
Plain language summary
Patients with distal Crohn’s disease often undergo colon resection with a stoma to divert the intestinal stream from the rectum in hopes of achieving sufficient healing to allow ultimate re-establishment of intestinal continuity. Patients and practitioners alike should be aware of the long-term success rates of this procedure. Our retrospective study of 197 patients found that half required later proctectomy and an additional one-quarter remained symptomatic with excluded rectums. Only 14% remained symptom-free after reanastomosis, and only 6% if perianal disease was the initial surgical indication. These data provide estimation of long-term surgical outcomes.
© The Author(s) 2022. Published by Oxford University Press on behalf of Crohn’s & Colitis Foundation. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
The authors have no conflicts of interest to disclose. The current manuscript, including related data and figures, has not been previously published and is not under consideration elsewhere.
Figures
Similar articles
-
Natural history of perianal Crohn's disease after fecal diversion.Inflamm Bowel Dis. 2014 Dec;20(12):2260-5. doi: 10.1097/MIB.0000000000000216. Inflamm Bowel Dis. 2014. PMID: 25230164
-
What Factors Are Associated With the Eventual Need for an Ileostomy After Total Abdominal Colectomy and Ileosigmoid or Ileorectal Anastomosis for Crohn's Colitis in the Biologic Era?Dis Colon Rectum. 2020 Apr;63(4):504-513. doi: 10.1097/DCR.0000000000001556. Dis Colon Rectum. 2020. PMID: 32015288
-
Fecal Diversion for Perianal Crohn Disease in the Era of Biologic Therapies: A Multicenter Study.Inflamm Bowel Dis. 2022 Feb 1;28(2):226-233. doi: 10.1093/ibd/izab086. Inflamm Bowel Dis. 2022. PMID: 33988225
-
Fecal Diversion in Complex Perianal Fistulizing Crohn's Disease.Clin Colon Rectal Surg. 2022 Jan 17;35(1):5-9. doi: 10.1055/s-0041-1740028. eCollection 2022 Jan. Clin Colon Rectal Surg. 2022. PMID: 35069025 Free PMC article. Review.
-
Diagnosis and treatment of fistulising Crohn's disease.Dan Med Bull. 2011 Oct;58(10):C4338. Dan Med Bull. 2011. PMID: 21975159 Review.
Cited by
-
Surgical treatment of inflammatory bowel disease: From the gastroenterologist's stand-point.World J Gastrointest Surg. 2024 May 27;16(5):1235-1254. doi: 10.4240/wjgs.v16.i5.1235. World J Gastrointest Surg. 2024. PMID: 38817292 Free PMC article.
-
A Guide Through the Tunnel: Updates in the Approach to Classification and Management of Perianal Fistulizing Crohn's Disease.Curr Gastroenterol Rep. 2025 Jun 27;27(1):46. doi: 10.1007/s11894-025-00998-0. Curr Gastroenterol Rep. 2025. PMID: 40576852 Review.
References
-
- Farmer RG, Whelan G, Fazio VW. Long-term follow-up of patients with Crohn’s disease. Relationship between the clinical pattern and prognosis. Gastroenterology. 1985;88:1818–1825. - PubMed
-
- Bernstein CN, Loftus EV Jr, Ng SC, et al. .; Epidemiology and Natural History Task Force of the International Organization for the Study of Inflammatory Bowel Disease (IOIBD). Hospitalisations and surgery in Crohn’s disease. Gut. 2012;61:622–629. - PubMed
-
- Gu J, Valente MA, Remzi FH, Stocchi L. Factors affecting the fate of faecal diversion in patients with perianal Crohn’s disease. Colorectal Dis. 2015;17:66–72. - PubMed
-
- Geoghegan JG, Carton E, O’Shea AM, et al. . Crohn’s colitis: the fate of the rectum. Int J Colorectal Dis. 1998;13:256–259. - PubMed
-
- Nordenvall C, Myrelid P, Ekbom A, et al. . Probability, rate and timing of reconstructive surgery following colectomy for inflammatory bowel disease in Sweden: a population-based cohort study. Colorectal Dis. 2015;17:882–890. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
