

Temozolomide Treatment Alters Mismatch Repair and Boosts Mutational Burden in Tumor and Blood of Colorectal Cancer Patients
- PMID: 35522273
- PMCID: PMC9394384
- DOI: 10.1158/2159-8290.CD-21-1434
Temozolomide Treatment Alters Mismatch Repair and Boosts Mutational Burden in Tumor and Blood of Colorectal Cancer Patients
Abstract
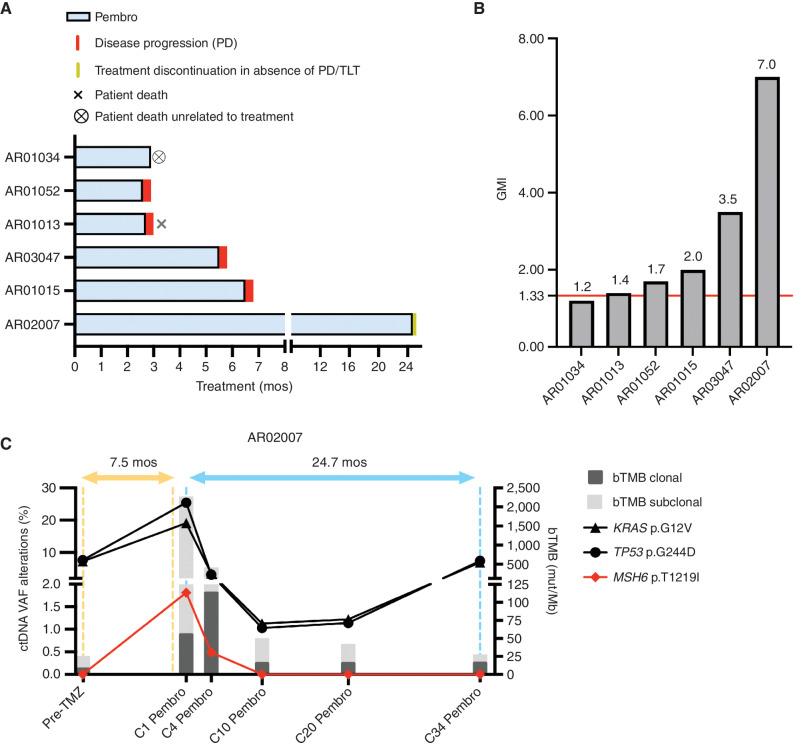
The majority of metastatic colorectal cancers (mCRC) are mismatch repair (MMR) proficient and unresponsive to immunotherapy, whereas MMR-deficient (MMRd) tumors often respond to immune-checkpoint blockade. We previously reported that the treatment of colorectal cancer preclinical models with temozolomide (TMZ) leads to MMR deficiency, increased tumor mutational burden (TMB), and sensitization to immunotherapy. To clinically translate these findings, we designed the ARETHUSA clinical trial whereby O6-methylguanine-DNA-methyltransferase (MGMT)-deficient, MMR-proficient, RAS-mutant mCRC patients received priming therapy with TMZ. Analysis of tissue biopsies and circulating tumor DNA (ctDNA) revealed the emergence of a distinct mutational signature and increased TMB after TMZ treatment. Multiple alterations in the nucleotide context favored by the TMZ signature emerged in MMR genes, and the p.T1219I MSH6 variant was detected in ctDNA and tissue of 94% (16/17) of the cases. A subset of patients whose tumors displayed the MSH6 mutation, the TMZ mutational signature, and increased TMB achieved disease stabilization upon pembrolizumab treatment.
Significance: MMR-proficient mCRCs are unresponsive to immunotherapy. We provide the proof of concept that inactivation of MMR genes can be achieved pharmacologically with TMZ and molecularly monitored in the tissue and blood of patients with mCRC. This strategy deserves additional evaluation in mCRC patients whose tumors are no longer responsive to standard-of-care treatments. See related commentary by Willis and Overman, p. 1612. This article is highlighted in the In This Issue feature, p. 1599.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures






Comment in
-
Inducing Hypermutability to Promote Anti-PD-1 Therapy Response.Cancer Discov. 2022 Jul 6;12(7):1612-1614. doi: 10.1158/2159-8290.CD-22-0492. Cancer Discov. 2022. PMID: 35791694 Free PMC article.
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin 2021;71:7–33. - PubMed
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–49. - PubMed
-
- Yoshino T, Arnold D, Taniguchi H, Pentheroudakis G, Yamazaki K, Xu RH, et al. Pan-Asian adapted ESMO consensus guidelines for the management of patients with metastatic colorectal cancer: a JSMO-ESMO initiative endorsed by CSCO, KACO, MOS, SSO and TOS. Ann Oncol 2018;29:44–70. - PubMed
-
- Benson AB, Venook AP, Al-Hawary MM, Arain MA, Chen YJ, Ciombor KK, et al. Colon cancer, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2021;19:329–59. - PubMed
-
- Sartore-Bianchi A, Trusolino L, Martino C, Bencardino K, Lonardi S, Bergamo F, et al. Dual-targeted therapy with trastuzumab and lapatinib in treatment-refractory, KRAS codon 12/13 wild-type, HER2-positive metastatic colorectal cancer (HERACLES): a proof-of-concept, multicentre, open-label, phase 2 trial. Lancet Oncol 2016;17:738–46. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
