

Alpha Variant Coronavirus Outbreak in a Nursing Home Despite High Vaccination Coverage: Molecular, Epidemiological, and Immunological Studies
- PMID: 35522980
- PMCID: PMC9129182
- DOI: 10.1093/cid/ciab1005
Alpha Variant Coronavirus Outbreak in a Nursing Home Despite High Vaccination Coverage: Molecular, Epidemiological, and Immunological Studies
Abstract
Background: Vaccination may control the coronavirus disease 2019 (COVID-19) pandemic, including in nursing homes where many high-risk people live. We conducted extensive outbreak investigations.
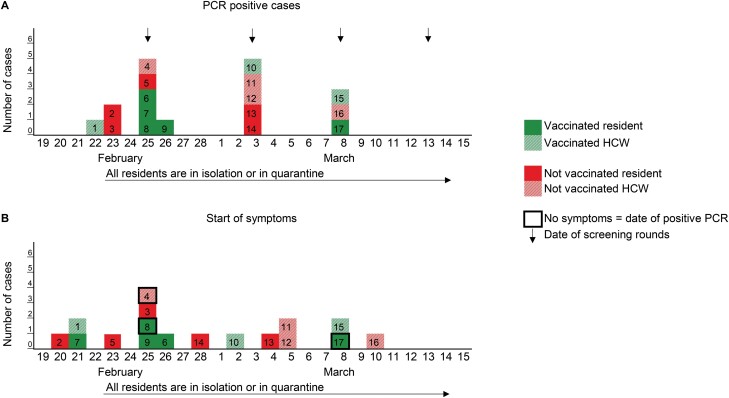
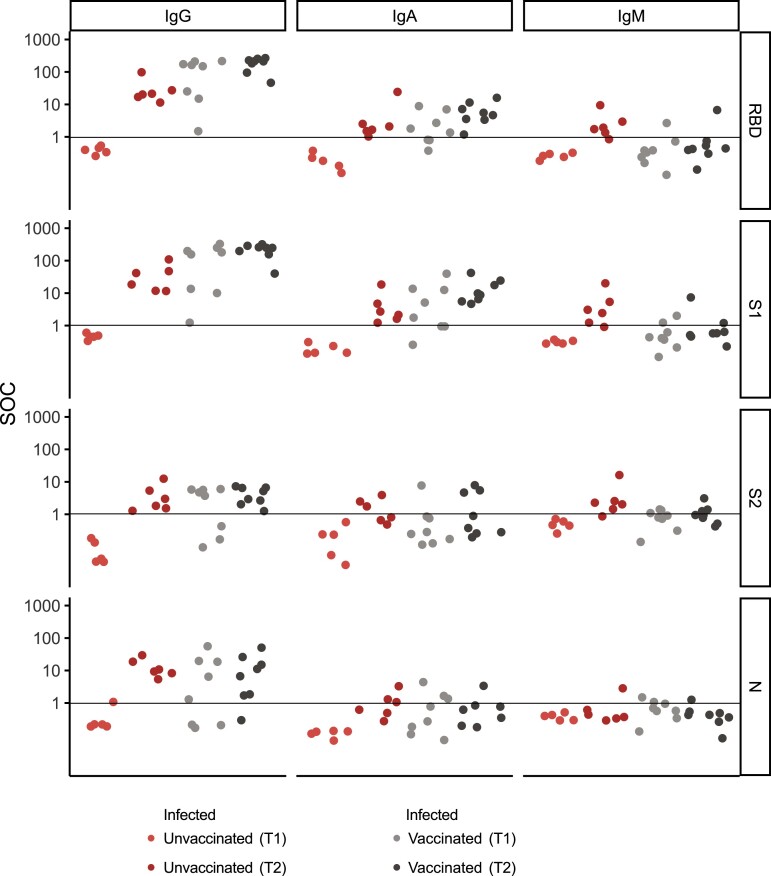
Methods: We studied an outbreak at a nursing home in Switzerland, where the uptake of messenger RNA vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was 82% among residents as of 21 January 2021. After diagnosis of COVID-19 in a vaccinated symptomatic healthcare worker (HCW) on 22 February, we performed outbreak investigations in house A (47 residents; 37 HCWs), using SARS-CoV-2-specific polymerase chain reaction testing of nasopharyngeal swab samples. We performed whole-genome sequencing of SARS-CoV-2 and serological analyses.
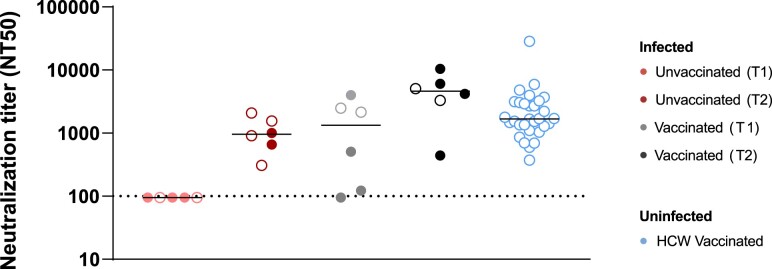
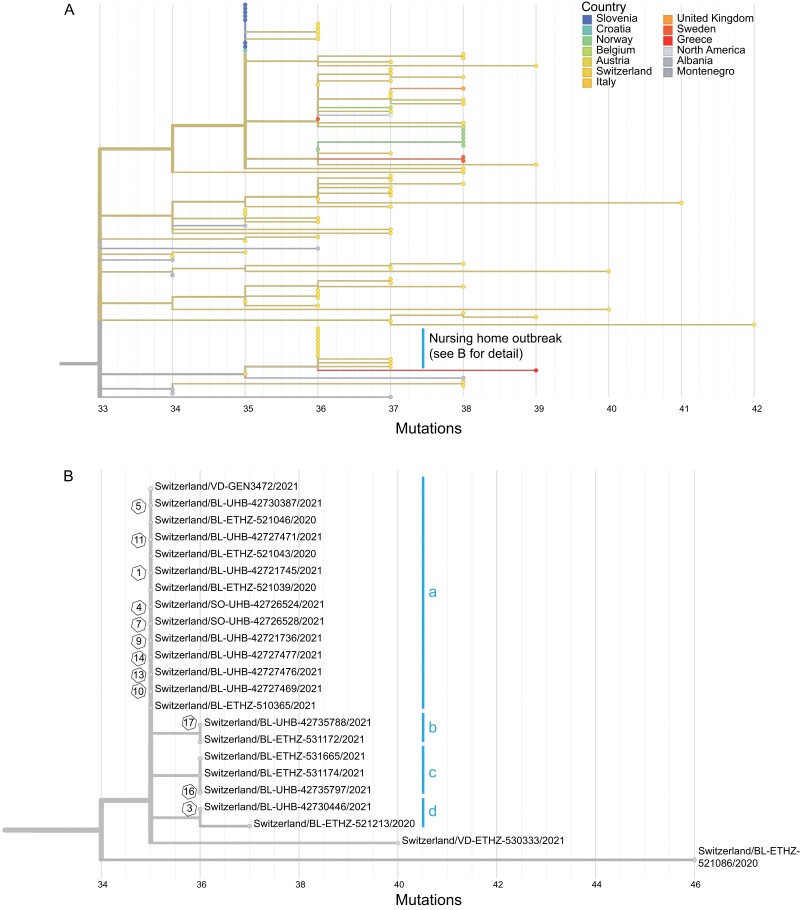
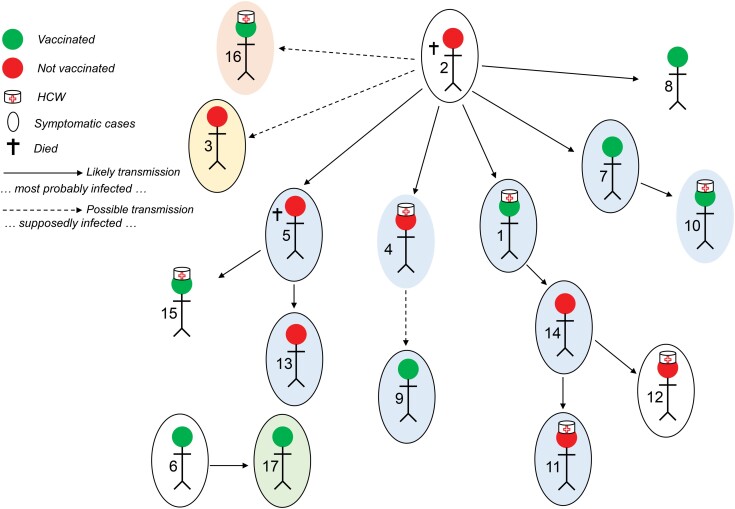
Results: We identified 17 individuals with positive polymerase chain reaction results, 10 residents (5 vaccinated) and 7 HCWs (3 vaccinated). The median age (interquartile range) was 86 (70-90) years among residents and 49 (29-59) years among HCWs. Of the 5 vaccinated residents, 3 had mild disease and 2 had no symptoms, whereas all 5 unvaccinated residents had mild to severe disease, and 2 died. Vaccine effectiveness for the prevention of infection among residents was 73.0% (95% confidence interval, 24.7%-90.1%). The 12 available genomes were all alpha variants. Neutralizing titers were significantly higher in vaccinated individuals on reexposure (>1 week after diagnosis) than in vaccinated, unexposed HCWs (P = .01). Transmission networks indicated 4 likely or possible transmissions from vaccinated to other individuals and 12 transmission events from unvaccinated individuals.
Conclusions: COVID-19 outbreaks can occur in nursing homes, including transmission from vaccinated persons to others. Outbreaks might occur silently, underlining the need for continued testing and basic infection control measures in these high-risk settings.
Keywords: B.1.1.7; COVID-19; Outbreak; UK variant; Vaccine; nursing home.
© The Author(s) 2022. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Conflict of interest statement
Figures
Similar articles
-
Epidemiology of COVID-19 outbreaks in aged care facilities during postvaccine period: a systematic review and meta-analysis.BMJ Open. 2024 Mar 14;14(3):e073555. doi: 10.1136/bmjopen-2023-073555. BMJ Open. 2024. PMID: 38485480 Free PMC article.
-
COVID-19 Outbreaks in Nursing Homes Despite Full Vaccination with BNT162b2 of a Majority of Residents.Gerontology. 2022;68(12):1384-1392. doi: 10.1159/000523701. Epub 2022 Mar 21. Gerontology. 2022. PMID: 35313315 Free PMC article.
-
Outbreak of SARS-CoV-2 B.1.617.2 (delta) variant in a nursing home 28 weeks after two doses of mRNA anti-COVID-19 vaccines: evidence of a waning immunity.Clin Microbiol Infect. 2022 Apr;28(4):614.e5-614.e7. doi: 10.1016/j.cmi.2021.12.013. Epub 2021 Dec 24. Clin Microbiol Infect. 2022. PMID: 34958917 Free PMC article.
-
Investigation of an outbreak of symptomatic SARS-CoV-2 VOC 202012/01-lineage B.1.1.7 infection in healthcare workers, Italy.Clin Microbiol Infect. 2021 Aug;27(8):1174.e1-1174.e4. doi: 10.1016/j.cmi.2021.05.007. Epub 2021 May 10. Clin Microbiol Infect. 2021. PMID: 33984489 Free PMC article.
-
Postvaccination SARS-CoV-2 infection among healthcare workers: A systematic review and meta-analysis.J Med Virol. 2022 Apr;94(4):1428-1441. doi: 10.1002/jmv.27457. Epub 2021 Nov 24. J Med Virol. 2022. PMID: 34783055 Free PMC article.
Cited by
-
Epidemiological and Serological Analysis of a SARS-CoV-2 Outbreak in a Nursing Home: Impact of SARS-CoV-2 Vaccination and Enhanced Neutralizing Immunity Following Breakthrough Infection.Microorganisms. 2022 Sep 9;10(9):1809. doi: 10.3390/microorganisms10091809. Microorganisms. 2022. PMID: 36144413 Free PMC article.
-
Evaluation of In-Hospital Cluster of COVID-19 Associated With a Patient With Prolonged Viral Shedding Using Whole-Genome Sequencing.J Korean Med Sci. 2022 Oct 10;37(39):e289. doi: 10.3346/jkms.2022.37.e289. J Korean Med Sci. 2022. PMID: 36217571 Free PMC article.
-
Epidemiology of COVID-19 outbreaks in aged care facilities during postvaccine period: a systematic review and meta-analysis.BMJ Open. 2024 Mar 14;14(3):e073555. doi: 10.1136/bmjopen-2023-073555. BMJ Open. 2024. PMID: 38485480 Free PMC article.
References
-
- London School of Hygiene & Tropical Medicine. COVID-19 vaccine tracker. London, UK: London School of Hygiene & Tropical Medicine, 2020.. Available at: https://vac-lshtm.shinyapps.io/ncov_vaccine_landscape/. Accessed June 2021.
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
