

Medial patellofemoral ligament is a part of the vastus medialis obliquus and vastus intermedius aponeuroses attaching to the medial epicondyle
- PMID: 35523877
- PMCID: PMC9568457
- DOI: 10.1007/s00167-022-06984-7
Medial patellofemoral ligament is a part of the vastus medialis obliquus and vastus intermedius aponeuroses attaching to the medial epicondyle
Abstract
Purpose: This study aimed to investigate the bony surface characteristic of the femoral attachment of the medial patellofemoral ligament (MPFL) and the correlation between the relevant layered structures, including muscular aponeurosis and the joint capsule, which contribute to patellofemoral joint (PFJ) stability.
Methods: The morphology of the medial aspect of the medial condyle using micro-computed tomography and analysed cortical bone thickening in 24 knees was observed. For the macroscopic and histological analyses, 21 and 3 knees were allocated, respectively. The Kruskal-Wallis one-way analysis of variance test with Dunn post hoc testing was performed for statistical analysis.
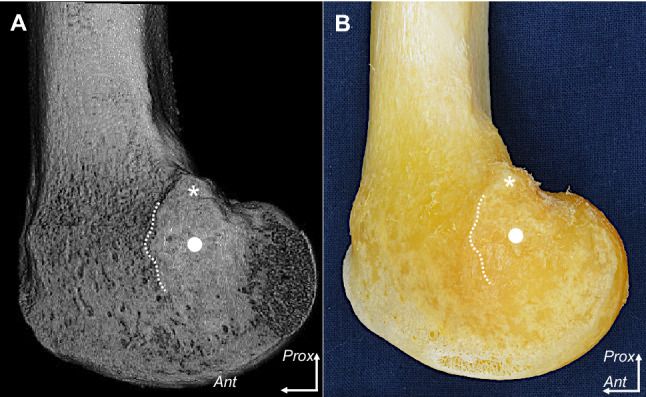
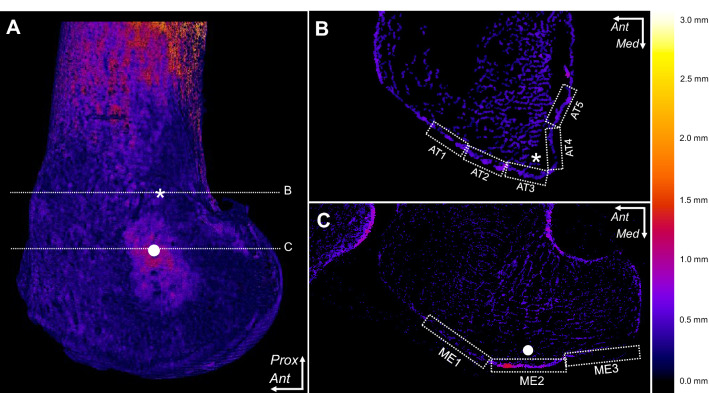
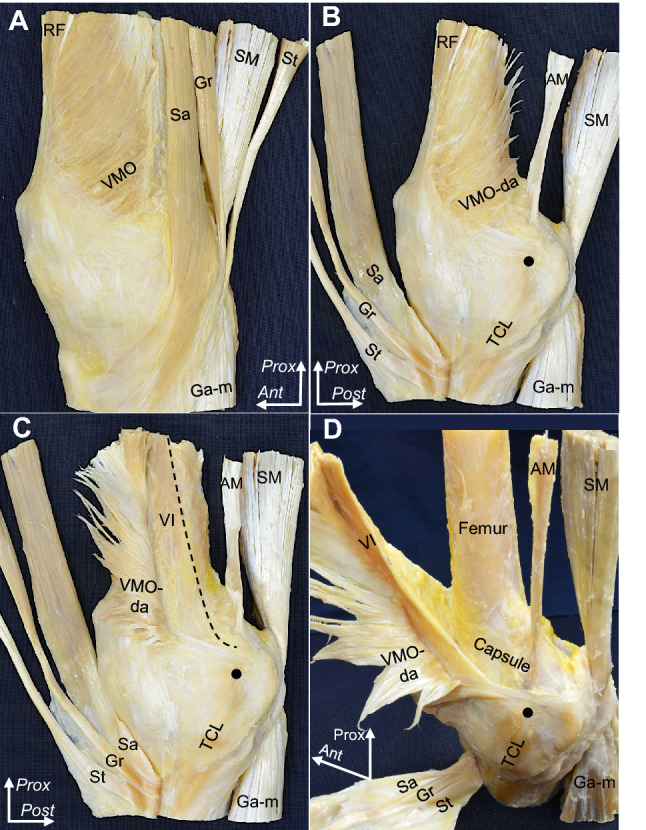
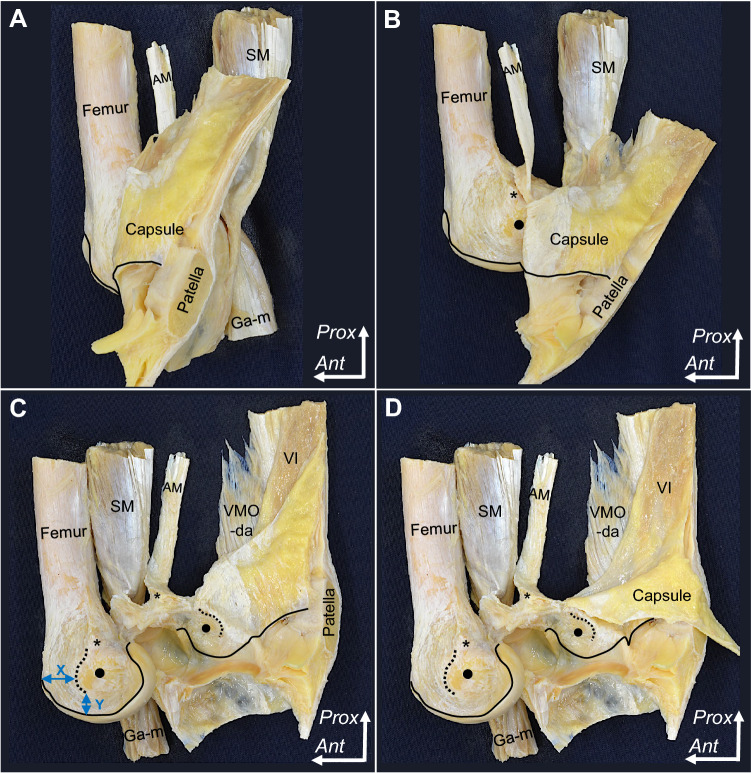
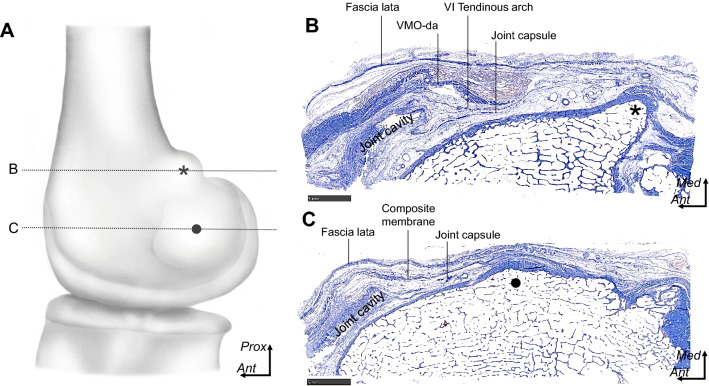
Results: At the level of the adductor tubercle, there were no significant differences in cortical bone thickness. At the level of the medial epicondyle (MEC), cortical bone thickness was considerably greater than that in other areas of the medial condyle (mean ± standard deviation, 0.60 ± 0.20 mm; p < 0.0001). Macroscopic analysis revealed that the deep aponeurosis of the vastus medialis obliquus and the tendinous arch of the vastus intermedius distally formed the composite membrane and adjoined to the joint capsule to firmly attach to MEC, which was located at 41.3 ± 5.7 mm posterior and 14.2 ± 3.1 mm superior to the joint cartilage. Histological analysis showed a composite membrane and adjoining capsule attached to MEC via fibrocartilage.
Conclusion: MPFL could be interpreted as part of the deep aponeurosis of the vastus medialis obliquus (VMO) and the tendinous arch of the vastus intermedius, which combined with the joint capsule to attach to MEC. The cortical bone thickening indicated that the tensile stresses were loaded on MEC in aged cadavers. Involvement of VMO and vastus intermedius aponeuroses in restored graft of MPFL could utilise the dynamic stability of surrounding muscles to mimic a native structure.
Keywords: Adductor tubercle; Aponeurosis; Cortical bone thickness; Joint capsule; Medial epicondyle; Medial patellofemoral ligament; Vastus intermedius; Vastus medialis obliquus.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Shape and size of the medial patellofemoral ligament for the best surgical reconstruction: a human cadaveric study.Knee Surg Sports Traumatol Arthrosc. 2014 Oct;22(10):2327-33. doi: 10.1007/s00167-014-3207-y. Epub 2014 Aug 17. Knee Surg Sports Traumatol Arthrosc. 2014. PMID: 25129113
-
Cadaveric Study to Define the Anatomy of the Medial Patellofemoral Ligament (MPFL) and Its Variant Patterns.Cureus. 2023 May 22;15(5):e39333. doi: 10.7759/cureus.39333. eCollection 2023 May. Cureus. 2023. PMID: 37351230 Free PMC article.
-
Anatomic study of the attachment of the medial patellofemoral ligament and its characteristic relationships to the vastus intermedius.Knee Surg Sports Traumatol Arthrosc. 2013 Feb;21(2):305-10. doi: 10.1007/s00167-012-1993-7. Epub 2012 Apr 11. Knee Surg Sports Traumatol Arthrosc. 2013. PMID: 22491706
-
Anatomy and biomechanics of the medial patellofemoral ligament.Knee. 2003 Sep;10(3):215-20. doi: 10.1016/s0968-0160(03)00006-1. Knee. 2003. PMID: 12893142 Review.
-
Recognition of evolving medial patellofemoral anatomy provides insight for reconstruction.Knee Surg Sports Traumatol Arthrosc. 2019 Aug;27(8):2537-2550. doi: 10.1007/s00167-018-5266-y. Epub 2018 Oct 28. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 30370440 Review.
Cited by
-
Novel combination method of wide-range serial sectioning and 3D reconstruction visualizing both macro-level dynamics and micro-level interactions in an attempt to analyze the female pelvic floor.Anat Sci Int. 2023 Jul;98(3):343-352. doi: 10.1007/s12565-023-00710-0. Epub 2023 Mar 7. Anat Sci Int. 2023. PMID: 36882587 Free PMC article. Review.
-
Medial Patellofemoral Ligament Reconstruction With Quadriceps Tendon Using an Expanding PEEK Anchor.Arthrosc Tech. 2025 Apr 2;14(6):103531. doi: 10.1016/j.eats.2025.103531. eCollection 2025 Jun. Arthrosc Tech. 2025. PMID: 40656693 Free PMC article.
-
Anterior Attachments of the Medial Patellofemoral Ligament: Morphological Characteristics.J Bone Joint Surg Am. 2025 Apr 2;107(7):741-748. doi: 10.2106/JBJS.24.00332. Epub 2025 Feb 21. J Bone Joint Surg Am. 2025. PMID: 39983008 Free PMC article.
-
Anatomical study for elucidating the stabilization mechanism in the trapeziometacarpal joint.Sci Rep. 2022 Dec 1;12(1):20790. doi: 10.1038/s41598-022-25355-3. Sci Rep. 2022. PMID: 36456627 Free PMC article.
-
Posteromedial capsular anatomy of the tibia for consideration of the medial meniscal support structure using a multidimensional analysis.Sci Rep. 2023 Jul 25;13(1):12030. doi: 10.1038/s41598-023-38994-x. Sci Rep. 2023. PMID: 37491561 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
