

A novel non-invasive method of measuring microcirculatory perfusion and blood velocity in infants: a pilot study
- PMID: 35523975
- PMCID: PMC9076848
- DOI: 10.1038/s41598-022-10911-8
A novel non-invasive method of measuring microcirculatory perfusion and blood velocity in infants: a pilot study
Abstract
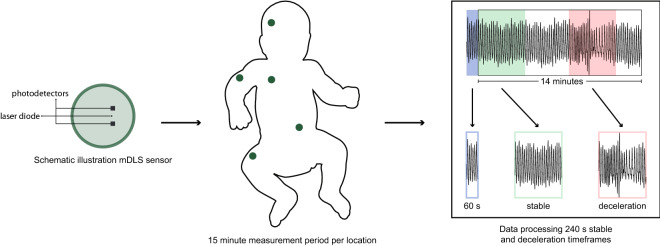
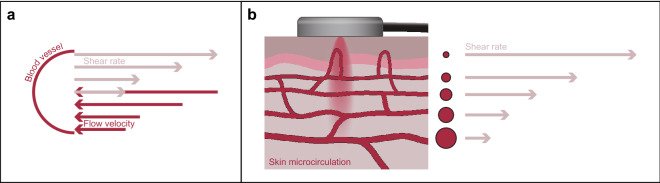
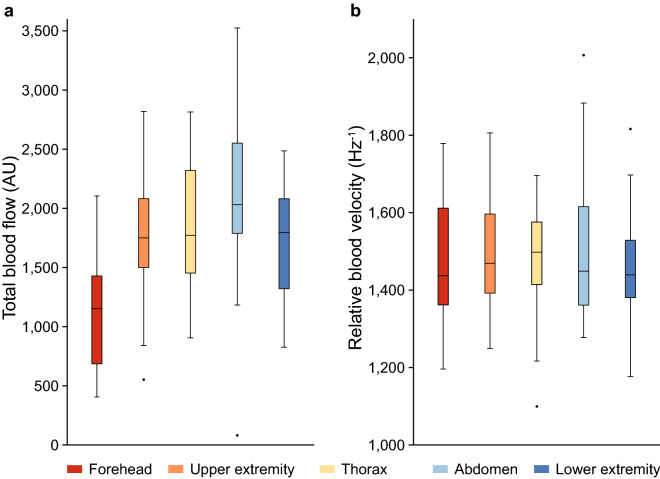
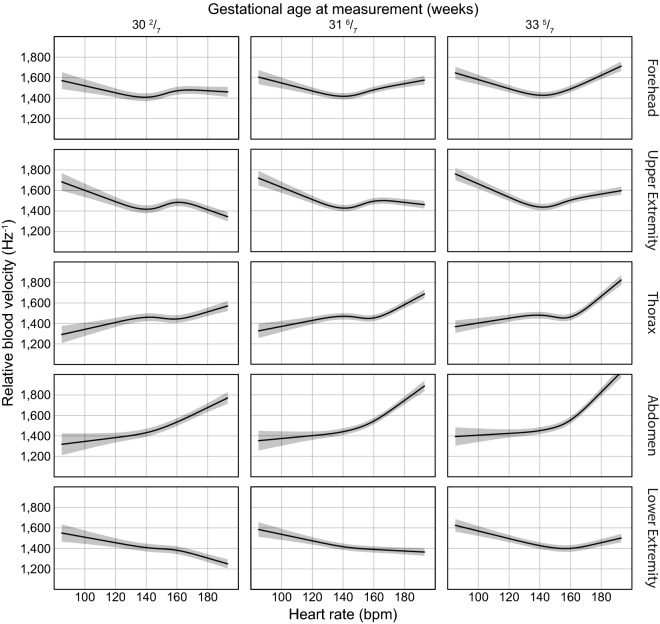
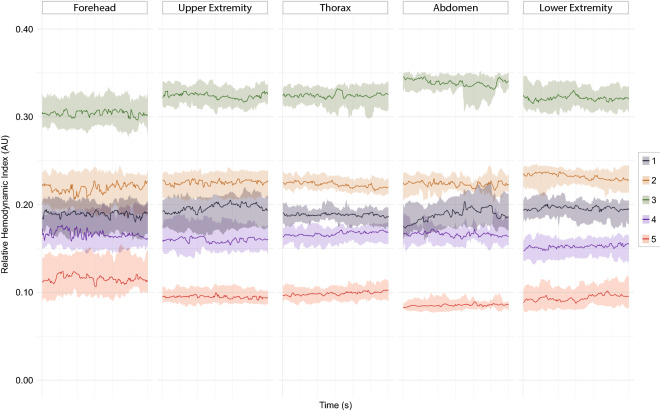
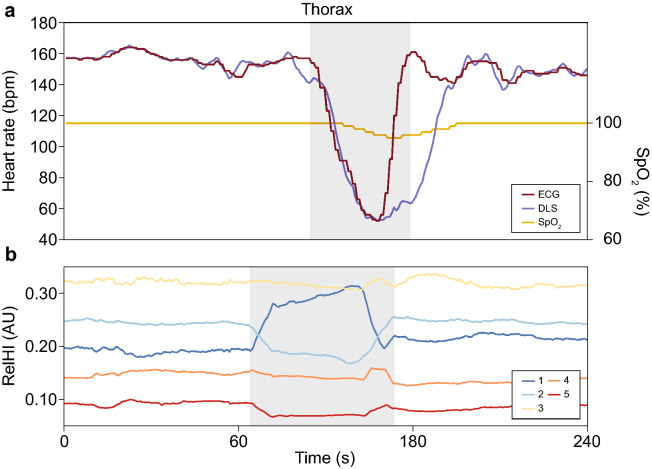
Current haemodynamic monitoring is mainly aimed at the macrocirculation. Multiple studies have demonstrated the importance of the microcirculation in relation to the patient's condition and impact of treatment strategies. However, continuous monitoring of the microcirculation is not yet possible in the neonatal field. A novel dynamic light scattering (DLS) sensor technology for continuous monitoring of the microcirculation was investigated in the neonatal population. Thirty-one haemodynamically stable infants were included. Sequential measurements at the forehead, upper extremity, thorax, abdomen and lower extremity were conducted with the DLS sensor. For analyses stable measurements were selected. The DLS parameters, total blood flow (TBF) and relative blood velocity (RBV), were compared between measurement locations. Changes in relative haemodynamic indices (relHIs), indicating the distribution of blood flow in the microcirculatory blood vessels, were associated with heart rate decelerations. Measurements performed at the forehead had significantly lower TBF levels, compared to measurements at other locations. Early changes in relHIs around a heart rate deceleration were recorded a median (IQR) of 22.0 (13.5-27.0) s before the onset. Measurement of the currently unavailable parameters TBF, RBV and relHIs is possible with DLS technology. Validation of the DLS technology is needed for clinical implementation.
© 2022. The Author(s).
Conflict of interest statement
IF is CEO of Elfi-Tech Ltd. The other authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
