

Image-guided navigation for locally advanced primary and locally recurrent rectal cancer: evaluation of its early cost-effectiveness
- PMID: 35524234
- PMCID: PMC9074374
- DOI: 10.1186/s12885-022-09561-w
Image-guided navigation for locally advanced primary and locally recurrent rectal cancer: evaluation of its early cost-effectiveness
Abstract
Background: A first pilot study showed that an image-guided navigation system could improve resection margin rates in locally advanced (LARC) and locally recurrent rectal cancer (LRRC) patients. Incremental surgical innovation is often implemented without reimbursement consequences, health economic aspects should however also be taken into account. This study evaluates the early cost-effectiveness of navigated surgery compared to standard surgery in LARC and LRRC.
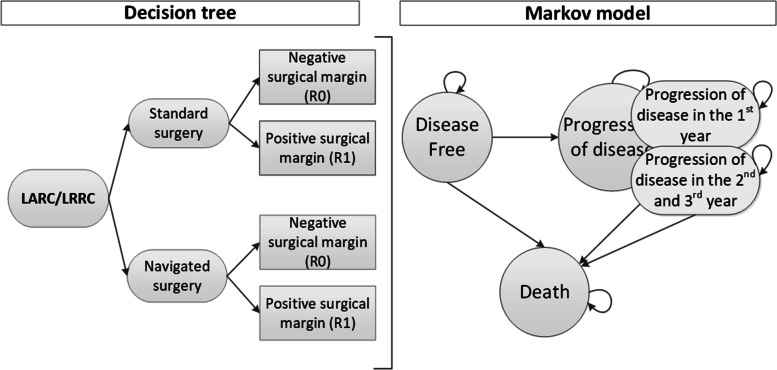
Methods: A Markov decision model was constructed to estimate the expected costs and outcomes for navigated and standard surgery. The input parameters were based on pilot data from a prospective (navigation cohort n = 33) and retrospective (control group n = 142) data. Utility values were measured in a comparable group (n = 63) through the EQ5D-5L. Additionally, sensitivity and value of information analyses were performed.
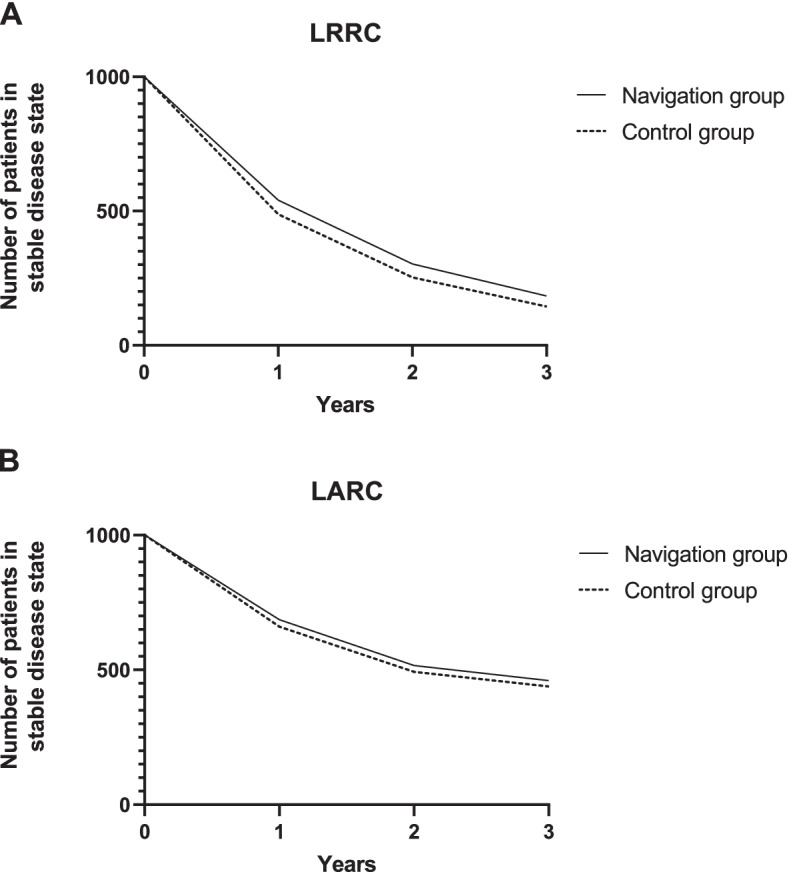
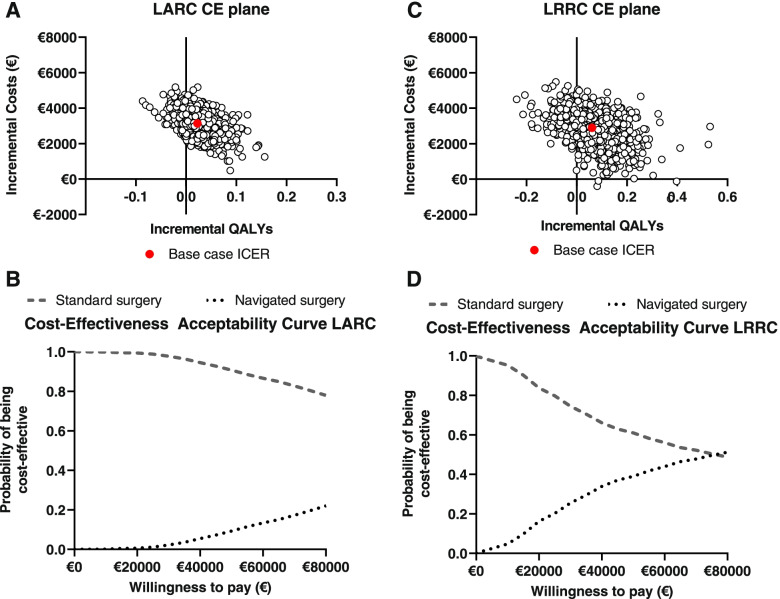
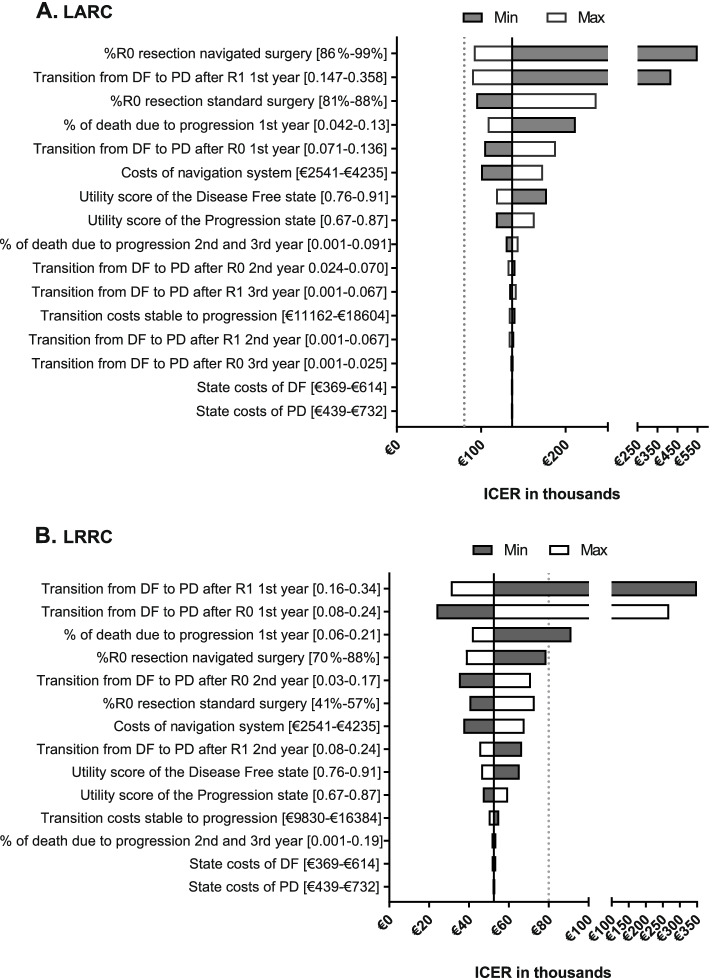
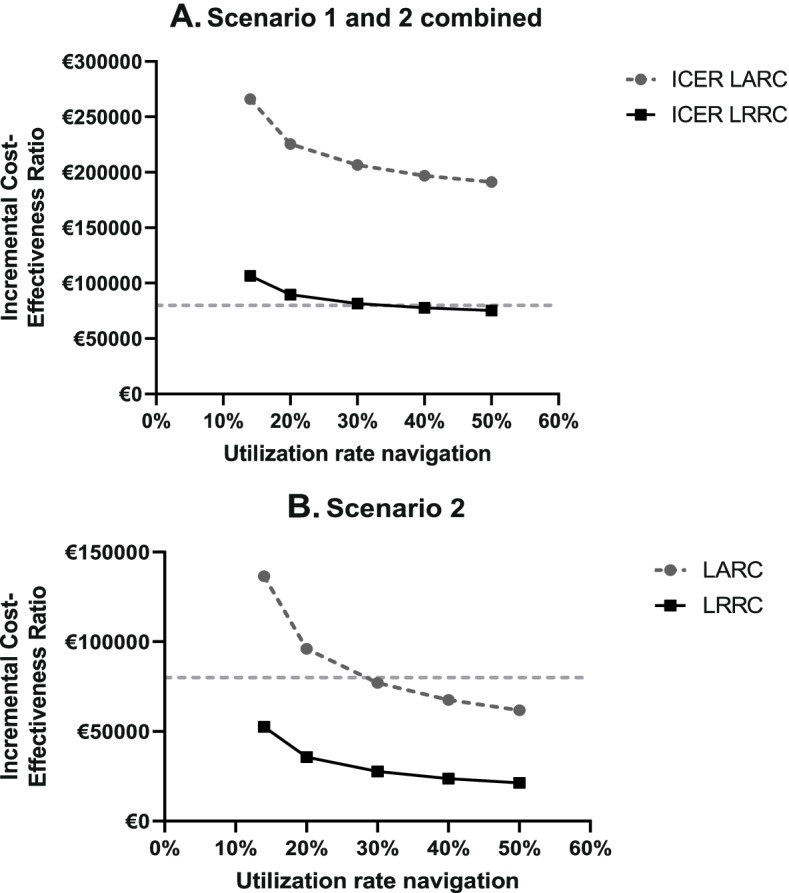
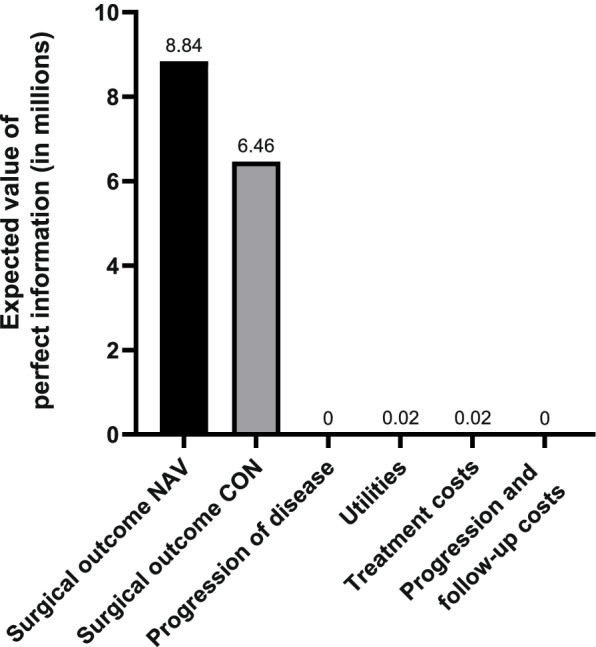
Results: Based on this early evaluation, navigated surgery showed incremental costs of €3141 and €2896 in LARC and LRRC. In LARC, navigated surgery resulted in 2.05 Quality-Adjusted Life Years (QALYs) vs 2.02 QALYs for standard surgery. For LRRC, we found 1.73 vs 1.67 QALYs respectively. This showed an Incremental Cost-Effectiveness Ratio (ICER) of €136.604 for LARC and €52.510 for LRRC per QALY gained. In scenario analyses, optimal utilization rates of the navigation technology lowered the ICER to €61.817 and €21.334 for LARC and LRRC. The ICERs of both indications were most sensitive to uncertainty surrounding the risk of progression in the first year after surgery, the risk of having a positive surgical margin, and the costs of the navigation system.
Conclusion: Adding navigation system use is expected to be cost-effective in LRRC and has the potential to become cost-effective in LARC. To increase the probability of being cost-effective, it is crucial to optimize efficient use of both the hybrid OR and the navigation system and identify subgroups where navigation is expected to show higher effectiveness.
Keywords: Early cost-effectiveness analysis; Early health technology assessment; Local recurrent rectal cancer; Locally advanced rectal cancer; Navigation technology; Surgery.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Ned Tijdschr Geneeskd. Behandeling van lokaal recidiverend rectumcarcinoom. 2015;159;A8199. - PubMed
-
- Integraal Kankercentrum Nederland. Darmkanker in Nederland: cijfers uit de Nederlandse Kankerregistratie. https://www.iknl.nl/nieuws/2019/darmkanker-in-nederland-cijfers-uit-de-n.... Accessed 4 Feb 2020.
MeSH terms
LinkOut - more resources
Full Text Sources
