

Socioeconomic inequalities in stillbirth and neonatal mortality rates: evidence on Particularly Vulnerable Tribal Groups in eastern India
- PMID: 35524273
- PMCID: PMC9074184
- DOI: 10.1186/s12939-022-01655-y
Socioeconomic inequalities in stillbirth and neonatal mortality rates: evidence on Particularly Vulnerable Tribal Groups in eastern India
Abstract
Background: Tribal peoples are among the most marginalised groups worldwide. Evidence on birth outcomes in these groups is scant. We describe inequalities in Stillbirth Rate (SBR), Neonatal Mortality Rate (NMR), and uptake of maternal and newborn health services between tribal and less disadvantaged groups in eastern India, and examine the contribution of poverty and education to these inequalities.
Methods: We used data from a demographic surveillance system covering a 1 million population in Jharkhand State (March 2017 - August 2019) to describe SBR, NMR, and service uptake. We used logistic regression analysis combined with Stata's adjrr-command to estimate absolute and relative inequalities by caste/tribe (comparing Particularly Vulnerable Tribal Groups (PVTG) and other Scheduled Tribes (ST) with the less marginalised Other Backward Class (OBC)/none, using the Indian government classification), and by maternal education and household wealth.
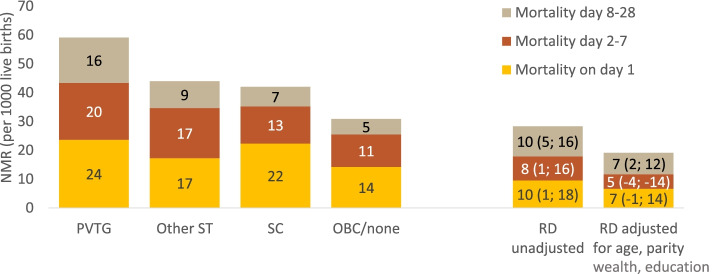
Results: PVTGs had a higher NMR (59/1000) than OBC/none (31/1000) (rate ratio (RR): 1.92, 95%CI: 1.55-2.38). This was partly explained by wealth and education, but inequalities remained large after adjustment (adjusted RR: 1.59, 95%CI: 1.28-1.98). NMR was also higher among other STs (44/1000), but disparities were smaller (RR: 1.47, 95%CI: 1.23-1.75). There was a systematic gradient in NMR by maternal education and household wealth. SBRs were only higher in poorer groups (RRpoorest vs. least poor:1.56, 95%CI: 1.14-2.13). Uptake of facility-based services was low among PVTGs (e.g. institutional birth: 25% vs. 69% in OBC/none) and among poorer and less educated women. However, 65% of PVTG women with an institutional birth used a maternity vehicle vs. 34% among OBC/none. Visits from frontline workers (Accredited Social Health Activists [ASHAs]) were similar across groups, and ASHA accompaniment of institutional births was similar across caste/tribe groups, and higher among poorer and less educated women. Attendance in participatory women's groups was similar across caste/tribe groups, and somewhat higher among richer and better educated women.
Conclusions: PVTGs are highly disadvantaged in terms of birth outcomes. Targeted interventions that reduce geographical barriers to facility-based care and address root causes of high poverty and low education in PVTGs are a priority. For population-level impact, they are to be combined with broader policies to reduce socio-economic mortality inequalities. Community-based interventions reach disadvantaged groups and have potential to reduce the mortality gap.
Keywords: India; Indigenous health; Inequalities; Maternity care; Neonatal mortality; Stillbirth.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Effect of participatory women's groups facilitated by Accredited Social Health Activists on birth outcomes in rural eastern India: a cluster-randomised controlled trial.Lancet Glob Health. 2016 Feb;4(2):e119-28. doi: 10.1016/S2214-109X(15)00287-9. Lancet Glob Health. 2016. PMID: 26823213 Clinical Trial.
-
How equitable is the uptake of conditional cash transfers for maternity care in India? Evidence from the Janani Suraksha Yojana scheme in Odisha and Jharkhand.Int J Equity Health. 2017 Mar 10;16(1):48. doi: 10.1186/s12939-017-0539-5. Int J Equity Health. 2017. PMID: 28283045 Free PMC article.
-
Wealth and education-related inequalities in the utilisation of reproductive, maternal, newborn, and child health interventions within scheduled tribes in India: an analysis of Odisha and Jharkhand.BMC Public Health. 2024 Jun 17;24(1):1605. doi: 10.1186/s12889-024-18857-4. BMC Public Health. 2024. PMID: 38886705 Free PMC article.
-
Health status of particularly vulnerable tribal groups (PVTGs) of Odisha: a narrative review.J Health Popul Nutr. 2024 Oct 30;43(1):176. doi: 10.1186/s41043-024-00671-8. J Health Popul Nutr. 2024. PMID: 39478584 Free PMC article. Review.
-
Impact of health literacy on pregnancy outcomes in socioeconomically disadvantaged and ethnic minority populations: A scoping review.Int J Gynaecol Obstet. 2025 Jan;168(1):69-81. doi: 10.1002/ijgo.15852. Epub 2024 Aug 22. Int J Gynaecol Obstet. 2025. PMID: 39175268 Free PMC article.
Cited by
-
Pregnancy outcomes among Indian women: increased prevalence of miscarriage and stillbirth during 2015-2021.BMC Pregnancy Childbirth. 2023 Mar 8;23(1):150. doi: 10.1186/s12884-023-05470-3. BMC Pregnancy Childbirth. 2023. PMID: 36890450 Free PMC article.
-
Verbal autopsy to assess causes of mortality among the economically productive age group in the tribal region of Melghat, central India.Indian J Med Res. 2023 Sep;158(3):217-254. doi: 10.4103/ijmr.ijmr_3299_21. Indian J Med Res. 2023. PMID: 37861621 Free PMC article.
-
Uncovering the causes and socio-demographic constructs of stillbirths and neonatal deaths in an urban slum of Karachi.PLoS One. 2024 Apr 5;19(4):e0298120. doi: 10.1371/journal.pone.0298120. eCollection 2024. PLoS One. 2024. PMID: 38578771 Free PMC article.
-
Burden, Differentials and Causes of Stillbirths in India: A Systematic Review and Meta Analysis.Indian J Pediatr. 2023 Dec;90(Suppl 1):54-62. doi: 10.1007/s12098-023-04749-9. Epub 2023 Aug 9. Indian J Pediatr. 2023. PMID: 37556034
-
Stillbirths in India: Current Status, Challenges, and the Way Forward.Indian J Pediatr. 2023 Dec;90(Suppl 1):63-70. doi: 10.1007/s12098-023-04807-2. Epub 2023 Aug 22. Indian J Pediatr. 2023. PMID: 37605065 Review.
References
-
- Ministry of Tribal Affairs, Government of India. Annual Report 2020–2021. New Delhi: Ministry of Tribal Affairs, Government of India 2021. Available from: https://tribal.nic.in/downloads/Statistics/AnnualReport/AREnglish2021.pdf. Accessed 12 June 2021.
-
- Xaxa VR, Bara U, Misra J, Bang KK, Basant A, Panda S. H. Report of the High Level Committee on Socioeconomic, Health and Educational Status of Tribal Communities of India New Delhi: Ministry of Tribal Affairs 2014 May 2014. Available from: http://archive.indianstatistics.org/misc/xaxacommittee.pdf. Accessed 12 June 2021.
-
- World Health Organization. Newborns: Improving survival and well-being Geneva: World Health Organisation; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/newborns-reducing-morta.... Accessed 20 May 2021.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
