

Efficacy and safety of anlotinib with and without EGFR-TKIs or immunotherapy in the treatment of elder patients with non-small-cell lung cancer: a retrospective study
- PMID: 35524294
- PMCID: PMC9074279
- DOI: 10.1186/s12890-022-01981-5
Efficacy and safety of anlotinib with and without EGFR-TKIs or immunotherapy in the treatment of elder patients with non-small-cell lung cancer: a retrospective study
Abstract
Background: Anlotinib is a multitarget tyrosine kinase inhibitor for treating patients with advanced non-small cell lung cancer (NSCLC). We aimed to assess the efficacy and safety of anlotinib in elder patients with advanced NSCLC.
Methods: Elder patients with advanced NSCLC who received anlotinib were enrolled. They were all age ≥ 65 years and with demonstrated records of EGFR gene status. All patients had received treatment with anlotinib or immune checkpoint inhibitors (ICIs)/EGFR-TKIs. The efficacy was evaluated according to the efficacy evaluation criteria for solid tumors (RECIST 1.1). Common Adverse Events Evaluation Criteria (CTCAE 4.03) were used to evaluate adverse drug reactions.
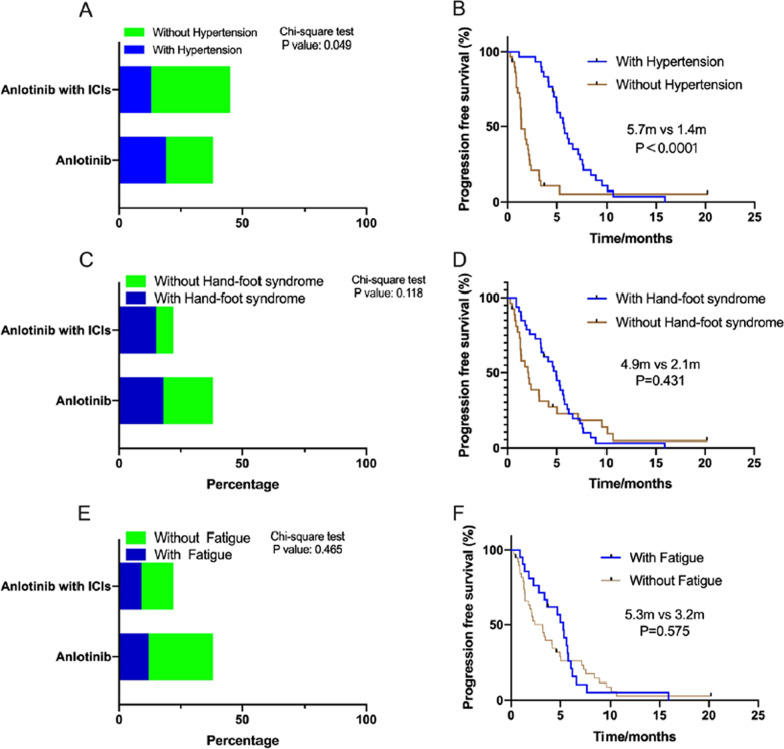
Results: A total of 91 patients were included in this study. We divided the patients into two groups (EGFR wild type: 60 patients; EGFR mutation: 31 patients). Among EGFR negative patients, the progression-free survival (PFS) for anlotinib monotherapy and anlotinib combination ICI therapy was 3.2 months and 5.0 months, respectively (P = 0.012). The difference in overall survival (OS) between monotherapy and combination therapy was also significant (9.5 vs. 18.4 months, respectively P = 0.010). Interestingly, we further analyzed differences between patients with hypertension and without hypertension, and found that hypertension was associated with better prognosis (5.7 vs. 1.4 months, P < 0.0001). In the EGFR mutation group, the PFS for anlotinib and EGFR-TKI combination treatment indicated better efficacy than that of anlotinib monotherapy (1.83 months vs. 7.03 months, respectively, P = 0.001). The median OS for monotherapy and combination therapy in the EGFR mutation group showed no statistical difference (28.34 months vs. 31.37 months, P = 0.223). The most common adverse reactions were hypertension, fatigue, and hand-foot syndrome, mainly of grade 1 or 2. No significant increase in adverse reactions was observed in patients ≥ 70 years of age.
Conclusions: Anlotinib treatment and combination regimens resulted in good efficacy and controllable adverse reactions in elder patients with advanced NSCLC.
Keywords: Angiogenesis; Non-small cell lung cancer; Prognosis; Tyrosine kinase inhibitors.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures




Similar articles
-
The later-line efficacy and safety of immune checkpoint inhibitors plus anlotinib in EGFR-mutant patients with EGFR-TKI-resistant NSCLC: a single-center retrospective study.Cancer Immunol Immunother. 2024 May 17;73(7):134. doi: 10.1007/s00262-024-03712-7. Cancer Immunol Immunother. 2024. PMID: 38758372 Free PMC article.
-
Efficacy and safety of anlotinib monotherapy or combination therapy in the treatment of patients with advanced non-small cell lung cancer: a retrospective real-world study conducted in East China.BMC Pulm Med. 2025 Apr 10;25(1):170. doi: 10.1186/s12890-025-03635-8. BMC Pulm Med. 2025. PMID: 40211232 Free PMC article.
-
Clinical outcomes and safety of osimertinib plus anlotinib for patients with previously treated EGFR T790M-positive NSCLC: A retrospective study.J Clin Pharm Ther. 2022 May;47(5):643-651. doi: 10.1111/jcpt.13591. Epub 2022 Jan 12. J Clin Pharm Ther. 2022. PMID: 35023208
-
China National Medical Products Administration approval summary: anlotinib for the treatment of advanced non-small cell lung cancer after two lines of chemotherapy.Cancer Commun (Lond). 2019 Jun 20;39(1):36. doi: 10.1186/s40880-019-0383-7. Cancer Commun (Lond). 2019. PMID: 31221221 Free PMC article. Review.
-
Aumolertinib: A Review in Non-Small Cell Lung Cancer.Drugs. 2022 Apr;82(5):577-584. doi: 10.1007/s40265-022-01695-2. Epub 2022 Mar 19. Drugs. 2022. PMID: 35305259 Review.
Cited by
-
Low‑dose anlotinib combined with EGFR‑TKI can be used as an alternative for EGFR‑TKI‑resistant non‑small cell lung cancer in elderly patients.Oncol Lett. 2023 Jun 13;26(2):323. doi: 10.3892/ol.2023.13909. eCollection 2023 Aug. Oncol Lett. 2023. PMID: 37415629 Free PMC article.
-
The pan-cancer analysis of LRG1 and its potential role in kidney renal clear cell carcinoma.RSC Med Chem. 2025 Feb 11. doi: 10.1039/d4md00940a. Online ahead of print. RSC Med Chem. 2025. PMID: 40008188 Free PMC article.
-
Anlotinib Plus Osimertinib in Osimertinib-Resistant Nonsquamous Nonsmall Cell Lung Cancer With Gradual Progression: A Retrospective Study.Thorac Cancer. 2025 May;16(10):e70071. doi: 10.1111/1759-7714.70071. Thorac Cancer. 2025. PMID: 40396214 Free PMC article.
-
Clinical Efficacy of Antianlotinib Combined with Immune Checkpoint Inhibitors in the Treatment of Advanced Non-Small-Cell Lung Cancer and Its Effect on Serum VEGF, CEA, and SCC-Ag.J Oncol. 2022 Oct 14;2022:1530875. doi: 10.1155/2022/1530875. eCollection 2022. J Oncol. 2022. PMID: 36276277 Free PMC article.
-
Research Progress on Mechanism and Management of Adverse Drug Reactions of Anlotinib.Drug Des Devel Ther. 2023 Nov 15;17:3429-3437. doi: 10.2147/DDDT.S426898. eCollection 2023. Drug Des Devel Ther. 2023. PMID: 38024530 Free PMC article. Review.
References
-
- Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Updated analysis of KEYNOTE-024: pembrolizumab versus platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor Proportion score of 50% or greater. J Clin Oncol. 2019;37(7):537–546. doi: 10.1200/JCO.18.00149. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
