

Frailty indices based on self-report, blood-based biomarkers and examination-based data in the Canadian Longitudinal Study on Aging
- PMID: 35524747
- PMCID: PMC9078045
- DOI: 10.1093/ageing/afac075
Frailty indices based on self-report, blood-based biomarkers and examination-based data in the Canadian Longitudinal Study on Aging
Abstract
Background: Frailty can be operationalised using the deficit accumulation approach, which considers health deficits across multiple domains. We aimed to develop, validate and compare three different frailty indices (FI) constructed from self-reported health measures (FI-Self Report), blood-based biomarkers (FI-Blood) and examination-based assessments (FI-Examination).
Methods: Up to 30,027 participants aged 45-85 years from the baseline (2011-2015) comprehensive cohort of the Canadian Longitudinal Study on Aging were included in the analyses. Following standard criteria, three FIs were created: a 48-item FI-Self Report, a 23-item FI-Blood and a 47-item FI-Examination. In addition a 118-item FI-Combined was constructed. Mortality status was ascertained in July 2019.
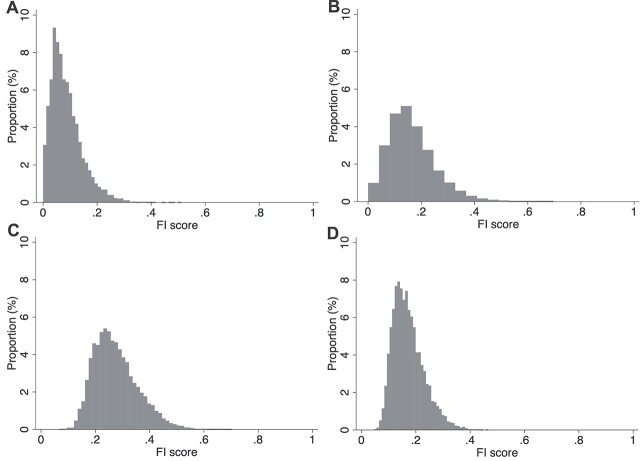
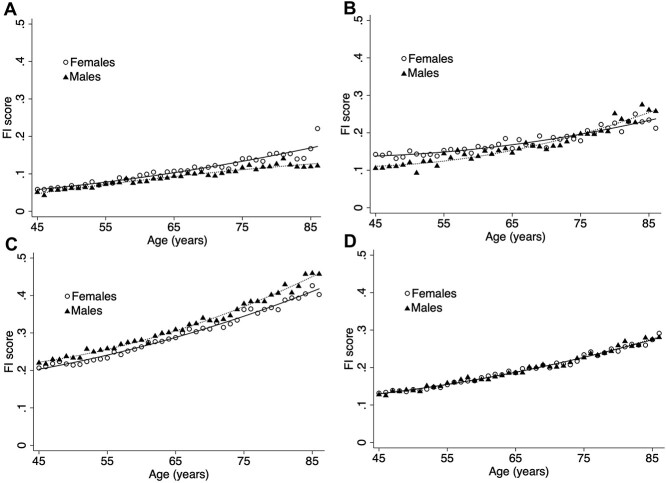
Results: FI-Blood and FI-Examination demonstrated broader distributions than FI-Self Report. FI-Self Report and FI-Blood scores were higher in females, whereas FI-Examination scores were higher in males. All FI scores increased nonlinearly with age and were highest at lower education levels. In sex and age-adjusted models, a 0.01 increase in FI score was associated with a 1.08 [95% confidence interval (CI): 1.07,1.10], 1.05 (1.04,1.06), 1.07 (1.05,1.08) and a 1.13 (1.11,1.16) increased odds of mortality for FI-Self Report, FI-Blood, FI-Examination and FI-Combined, respectively. Inclusion of the three distinct FI types in a single model yielded the best prognostic accuracy and model fit, even compared to the FI-Combined, with all FIs remaining independently associated with mortality.
Conclusion: Characteristics of all FIs were largely consistent with previously established FIs. To adequately capture frailty levels and to improve our understanding of the heterogeneity of ageing, FIs should consider multiple types of deficits including self-reported, blood and examination-based measures.
Keywords: Canadian Longitudinal Study on Aging (CLSA); Frailty; ageing; epidemiology; older people.
© The Author(s) 2022. Published by Oxford University Press on behalf of the British Geriatrics Society. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
Prognostic accuracy of 70 individual frailty biomarkers in predicting mortality in the Canadian Longitudinal Study on Aging.Geroscience. 2024 Jun;46(3):3061-3069. doi: 10.1007/s11357-023-01055-2. Epub 2024 Jan 6. Geroscience. 2024. PMID: 38182858 Free PMC article.
-
A frailty index based on laboratory deficits in community-dwelling men predicted their risk of adverse health outcomes.Age Ageing. 2016 Jul;45(4):463-8. doi: 10.1093/ageing/afw054. Epub 2016 Apr 13. Age Ageing. 2016. PMID: 27076524
-
Frailty differences across population characteristics associated with health inequality: a cross-sectional analysis of baseline data from the Canadian Longitudinal Study on Aging (CLSA).BMJ Open. 2021 Jul 19;11(7):e047945. doi: 10.1136/bmjopen-2020-047945. BMJ Open. 2021. PMID: 34281924 Free PMC article.
-
Development, validation and performance of laboratory frailty indices: A scoping review.Arch Gerontol Geriatr. 2023 Aug;111:104995. doi: 10.1016/j.archger.2023.104995. Epub 2023 Mar 11. Arch Gerontol Geriatr. 2023. PMID: 36963345
-
The frailty index based on laboratory test data as a tool to investigate the impact of frailty on health outcomes: a systematic review and meta-analysis.Age Ageing. 2023 Jan 8;52(1):afac309. doi: 10.1093/ageing/afac309. Age Ageing. 2023. PMID: 36626319 Free PMC article.
Cited by
-
Blood-based biomarkers for early frailty are sex-specific: validation of a combined in silico prediction and data-driven approach.Geroscience. 2025 Jun;47(3):3741-3758. doi: 10.1007/s11357-024-01449-w. Epub 2024 Dec 3. Geroscience. 2025. PMID: 39627572 Free PMC article.
-
Associations Between Deficit Accumulation Frailty and Baseline Markers of Lifestyle in the U.S. POINTER Trial.J Gerontol A Biol Sci Med Sci. 2025 Jan 16;80(2):glae279. doi: 10.1093/gerona/glae279. J Gerontol A Biol Sci Med Sci. 2025. PMID: 39549282 Free PMC article. Clinical Trial.
-
Gut microbial features and circulating metabolomic signatures of frailty in older adults.Nat Aging. 2024 Sep;4(9):1249-1262. doi: 10.1038/s43587-024-00678-0. Epub 2024 Jul 25. Nat Aging. 2024. PMID: 39054372
-
Prognostic accuracy of 70 individual frailty biomarkers in predicting mortality in the Canadian Longitudinal Study on Aging.Geroscience. 2024 Jun;46(3):3061-3069. doi: 10.1007/s11357-023-01055-2. Epub 2024 Jan 6. Geroscience. 2024. PMID: 38182858 Free PMC article.
-
Relationship between frailty and executive function by age and sex in the Canadian Longitudinal Study on Aging.Geroscience. 2025 Feb;47(1):1049-1060. doi: 10.1007/s11357-024-01256-3. Epub 2024 Jul 17. Geroscience. 2025. PMID: 39014131 Free PMC article.
References
-
- Rockwood K, Howlett SE. Age-related deficit accumulation and the diseases of ageing. Mech Ageing Dev 2019; 180: 107–16. - PubMed
-
- Rockwood K, Mitnitski A. Frailty, fitness, and the mathematics of deficit accumulation. Rev Clin Gerontol 2007; 17: 1–12.
