

Pharmacological treatment of major depressive disorder according to severity in psychiatric inpatients: results from the AMSP pharmacovigilance program from 2001-2017
- PMID: 35524828
- PMCID: PMC9217868
- DOI: 10.1007/s00702-022-02504-6
Pharmacological treatment of major depressive disorder according to severity in psychiatric inpatients: results from the AMSP pharmacovigilance program from 2001-2017
Abstract
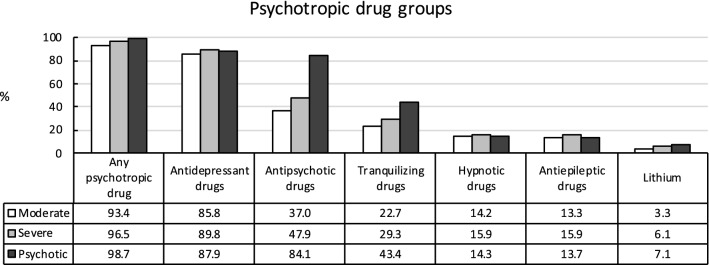
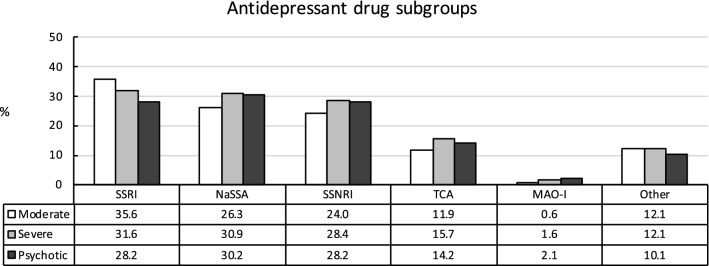
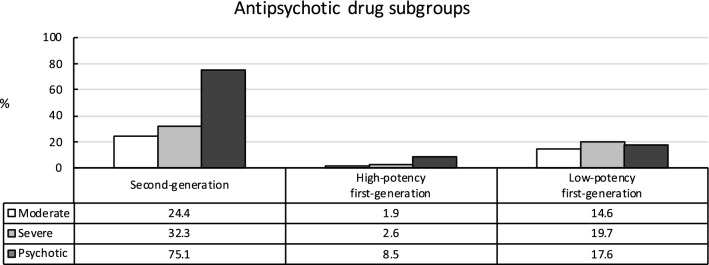
The International Classification of Diseases (10th Version) categorizes major depressive disorder (MDD) according to severity. Guidelines provide recommendations for the treatment of MDD according to severity. Aim of this study was to assess real-life utilization of psychotropic drugs based on severity of MDD in psychiatric inpatients. Drug utilization data from the program "Drug Safety in Psychiatry" (German: Arzneimittelsicherheit in der Psychiatrie, AMSP) were analyzed according to the severity of MDD. From 2001 to 2017, 43,868 psychiatric inpatients with MDD were treated in participating hospitals. Most patients were treated with ≥ 1 antidepressant drug (ADD; 85.8% of patients with moderate MDD, 89.8% of patients with severe MDD, and 87.9% of patients with psychotic MDD). More severely depressed patients were more often treated with selective serotonin-norepinephrine reuptake inhibitors and mirtazapine and less often with selective serotonin reuptake inhibitors (p < 0.001 each). Use of antipsychotic drugs (APDs), especially second-generation APDs, increased significantly with severity (37.0%, 47.9%, 84.1%; p < 0.001 each). APD + ADD was the most used combination (32.8%, 43.6%, 74.4%), followed by two ADDs (26.3%, 29.3%, 24.9%). Use of lithium was minimal (3.3%, 6.1% ,7.1%). The number of psychotropic drugs increased with severity of MDD-patients with psychotic MDD had the highest utilization of psychotropic drugs (93.4%, 96.5%, 98.7%; p < 0.001). ADD monotherapy was observed to a lesser extent, even in patients with non-severe MDD (23.2%, 17.1%, 4.4%). Findings reveal substantial discrepancies between guideline recommendations and real-life drug utilization, indicating that guidelines may insufficiently consider clinical needs within the psychiatric inpatient setting.
Keywords: Antidepressant drugs; Antipsychotic drugs; Major depressive disorder; Pharmacotherapy; Pharmacovigilance; Psychiatric inpatients.
© 2022. The Author(s).
Conflict of interest statement
JS took part in an educational event sponsored by Otsuka/Lundbeck. HM participated in an educational event sponsored by Livanova. ST is a member of the advisory board for Otsuka and Janssen-Cilag and has received speaker´s honoraria from Janssen-Cilag, Lundbeck/Otsuka, Recordati Pharma GmbH, and Servier. XB is currently working as Senior Manager for Takeda GmbH. All other authors state that they have no conflicts of interest to declare.
Figures
References
-
- Bauer M, Pfennig A, Severus E, Whybrow PC, Angst J, Möller HJ. World federation of societies of biological psychiatry (WFSBP) guidelines for biological treatment of unipolar depressive disorders, part 1: update 2013 on the acute and continuation treatment of unipolar depressive disorders. World J Biol Psychiatry. 2013;14(5):334–385. doi: 10.3109/15622975.2013.804195. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
