

Lung response to prone positioning in mechanically-ventilated patients with COVID-19
- PMID: 35526009
- PMCID: PMC9076814
- DOI: 10.1186/s13054-022-03996-0
Lung response to prone positioning in mechanically-ventilated patients with COVID-19
Abstract
Background: Prone positioning improves survival in moderate-to-severe acute respiratory distress syndrome (ARDS) unrelated to the novel coronavirus disease (COVID-19). This benefit is probably mediated by a decrease in alveolar collapse and hyperinflation and a more homogeneous distribution of lung aeration, with fewer harms from mechanical ventilation. In this preliminary physiological study we aimed to verify whether prone positioning causes analogue changes in lung aeration in COVID-19. A positive result would support prone positioning even in this other population.
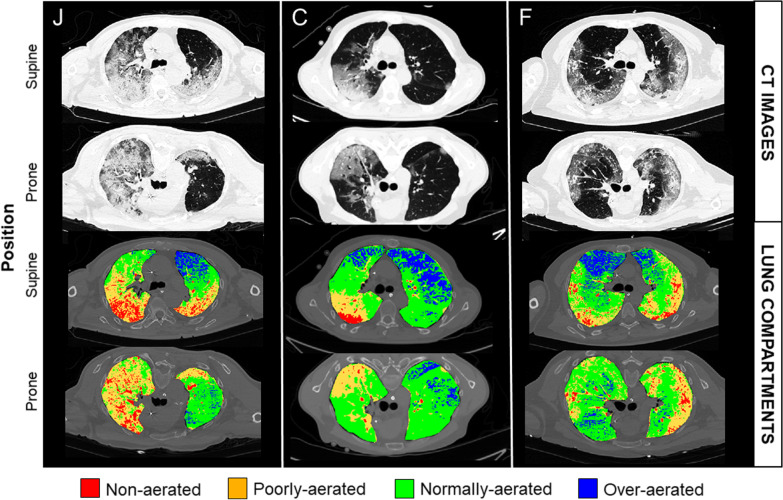
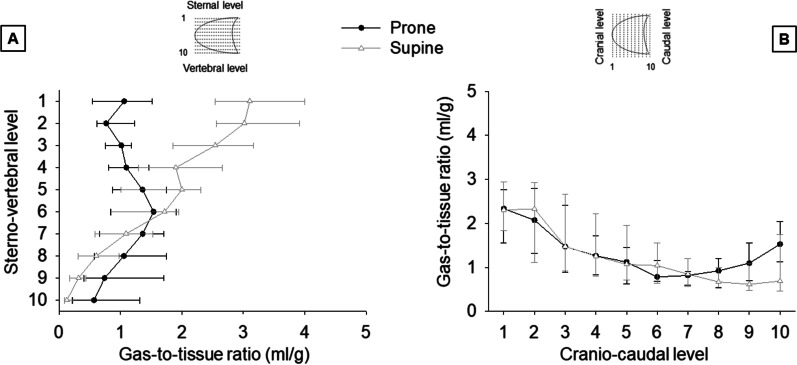
Methods: Fifteen mechanically-ventilated patients with COVID-19 underwent a lung computed tomography in the supine and prone position with a constant positive end-expiratory pressure (PEEP) within three days of endotracheal intubation. Using quantitative analysis, we measured the volume of the non-aerated, poorly-aerated, well-aerated, and over-aerated compartments and the gas-to-tissue ratio of the ten vertical levels of the lung. In addition, we expressed the heterogeneity of lung aeration with the standardized median absolute deviation of the ten vertical gas-to-tissue ratios, with lower values indicating less heterogeneity.
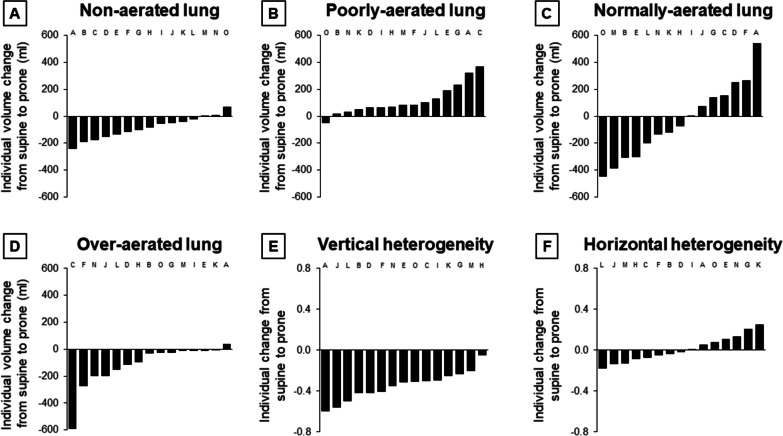
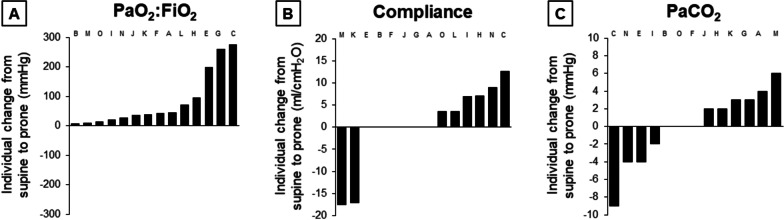
Results: By the time of the study, PEEP was 12 (10-14) cmH2O and the PaO2:FiO2 107 (84-173) mmHg in the supine position. With prone positioning, the volume of the non-aerated compartment decreased by 82 (26-147) ml, of the poorly-aerated compartment increased by 82 (53-174) ml, of the normally-aerated compartment did not significantly change, and of the over-aerated compartment decreased by 28 (11-186) ml. In eight (53%) patients, the volume of the over-aerated compartment decreased more than the volume of the non-aerated compartment. The gas-to-tissue ratio of the ten vertical levels of the lung decreased by 0.34 (0.25-0.49) ml/g per level in the supine position and by 0.03 (- 0.11 to 0.14) ml/g in the prone position (p < 0.001). The standardized median absolute deviation of the gas-to-tissue ratios of those ten levels decreased in all patients, from 0.55 (0.50-0.71) to 0.20 (0.14-0.27) (p < 0.001).
Conclusions: In fifteen patients with COVID-19, prone positioning decreased alveolar collapse, hyperinflation, and homogenized lung aeration. A similar response has been observed in other ARDS, where prone positioning improves outcome. Therefore, our data provide a pathophysiological rationale to support prone positioning even in COVID-19.
Keywords: Acute respiratory distress syndrome; Coronavirus disease 2019; Hypoxia; Mechanical ventilation; Pneumonia; Prone positioning.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Targeted lateral positioning decreases lung collapse and overdistension in COVID-19-associated ARDS.BMC Pulm Med. 2021 Apr 24;21(1):133. doi: 10.1186/s12890-021-01501-x. BMC Pulm Med. 2021. PMID: 33894747 Free PMC article.
-
Effect of decreasing PEEP on hyperinflation and collapse in COVID-19: A computed tomography study.Acta Anaesthesiol Scand. 2024 May;68(5):626-634. doi: 10.1111/aas.14401. Epub 2024 Feb 29. Acta Anaesthesiol Scand. 2024. PMID: 38425207
-
Prone positioning may increase lung overdistension in COVID-19-induced ARDS.Sci Rep. 2022 Oct 3;12(1):16528. doi: 10.1038/s41598-022-20881-6. Sci Rep. 2022. PMID: 36192569 Free PMC article.
-
Effect of prone positioning on oxygenation and static respiratory system compliance in COVID-19 ARDS vs. non-COVID ARDS.Respir Res. 2021 Aug 6;22(1):220. doi: 10.1186/s12931-021-01819-4. Respir Res. 2021. PMID: 34362368 Free PMC article. Review.
-
Prone positioning for ARDS patients-tips for preparation and use during the COVID-19 pandemic.Can J Anaesth. 2021 Apr;68(4):541-545. doi: 10.1007/s12630-020-01885-0. Epub 2020 Dec 24. Can J Anaesth. 2021. PMID: 33367994 Free PMC article. Review.
Cited by
-
Should We Encourage Prone Positioning in Patients With Non-Severe COVID-19?Chest. 2022 Oct;162(4):731-733. doi: 10.1016/j.chest.2022.06.031. Chest. 2022. PMID: 36210097 Free PMC article. No abstract available.
-
Prone Positioning for Patients With COVID-19-Induced Acute Hypoxemic Respiratory Failure: Flipping the Script.Respir Care. 2023 Oct;68(10):1449-1464. doi: 10.4187/respcare.11227. Respir Care. 2023. PMID: 37722733 Free PMC article. Review.
-
Exogenous surfactant reduces inflammation and redox imbalance in rats under prone or supine mechanical ventilation.Exp Biol Med (Maywood). 2023 Jun;248(12):1074-1084. doi: 10.1177/15353702231160352. Epub 2023 Apr 24. Exp Biol Med (Maywood). 2023. PMID: 37092748 Free PMC article.
-
Quantitative Computed Tomography and Response to Pronation in COVID-19 ARDS.Respir Care. 2024 Oct 25;69(11):1380-1391. doi: 10.4187/respcare.11625. Respir Care. 2024. PMID: 38594036
-
COVID-19-Related ARDS: Key Mechanistic Features and Treatments.J Clin Med. 2022 Aug 20;11(16):4896. doi: 10.3390/jcm11164896. J Clin Med. 2022. PMID: 36013135 Free PMC article. Review.
References
-
- Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195(9):1253–1263. doi: 10.1164/rccm.201703-0548ST. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
