

Trigger Point Injections
- PMID: 35526973
- PMCID: PMC9116734
- DOI: 10.1016/j.pmr.2022.01.011
Trigger Point Injections
Abstract
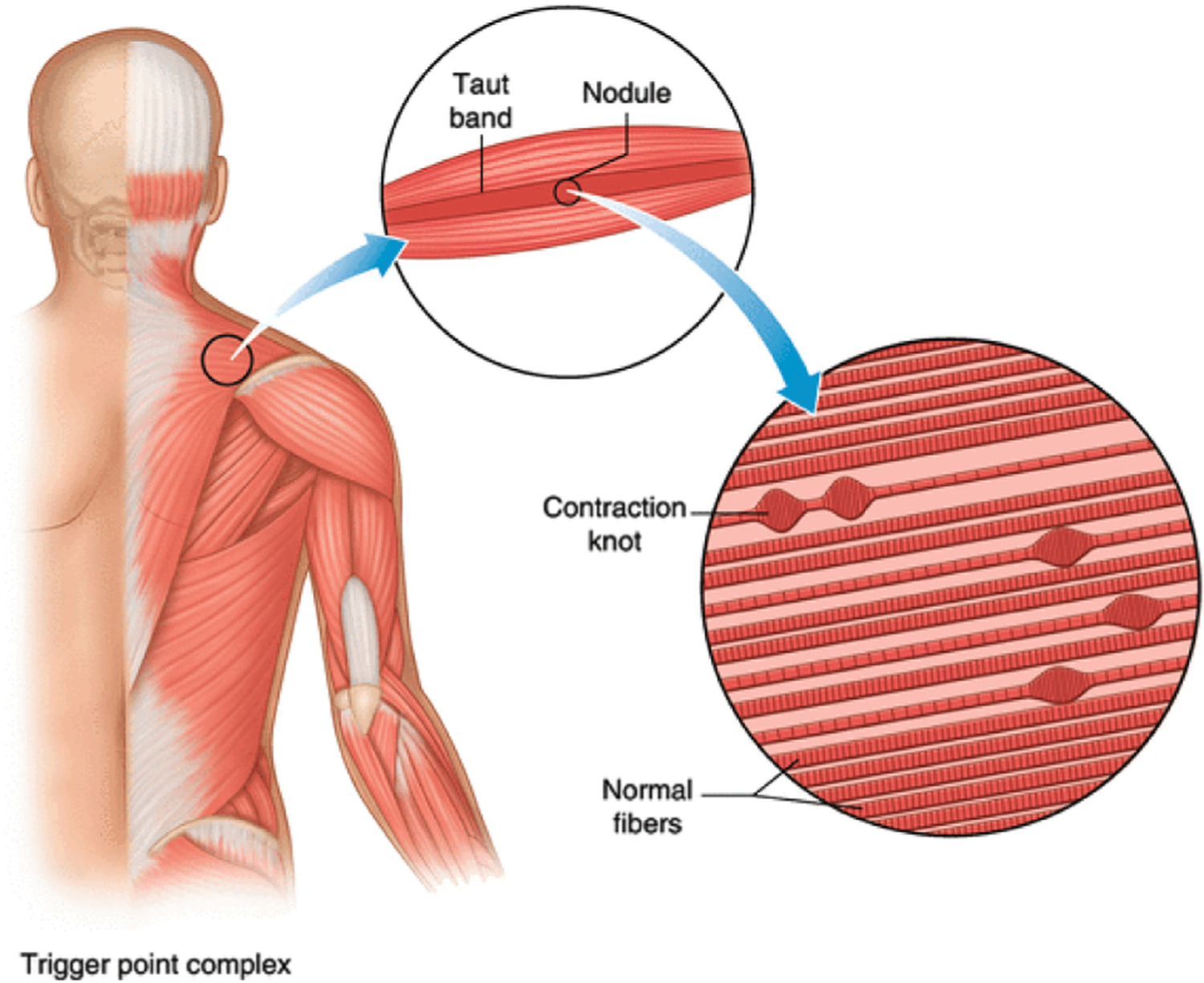
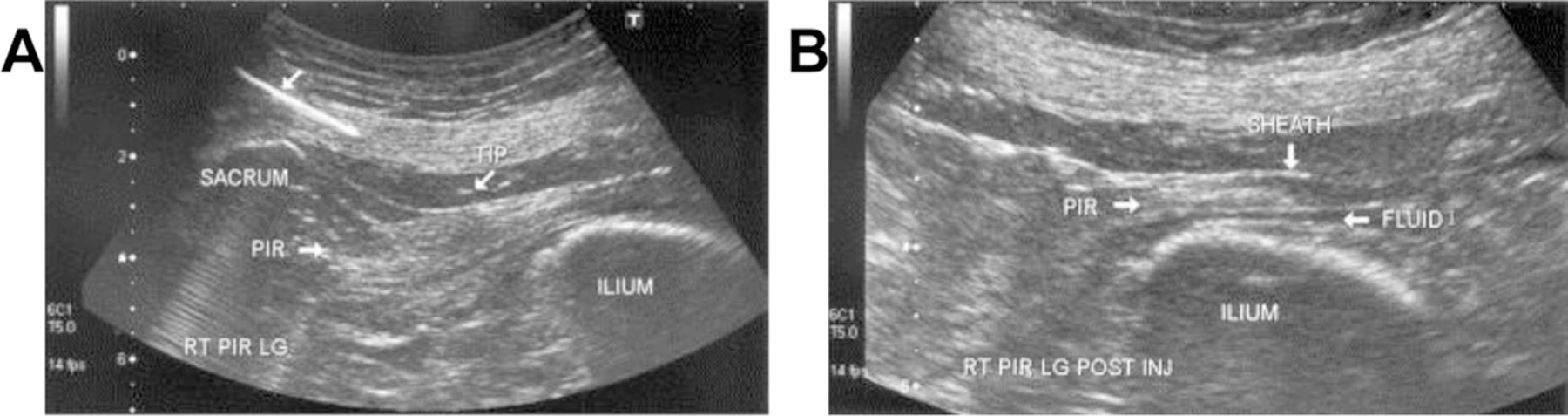
Myofascial pain and myofascial pain syndromes are among some of the most common acute and chronic pain conditions. Many interventional procedures can be performed in both an acute and chronic pain setting to address myofascial pain syndromes. Trigger point injections can be performed with or without imaging guidance such as fluoroscopy and ultrasound; however, the use of imaging in years past has been recommended to improve patient outcome and safety. Injections can be performed using no injectate (dry needling), or can involve the administration of local anesthetics, botulinum toxin, or corticosteroids.
Keywords: Botulinum toxin; Corticosteroid; Local anesthetic; Myofascial pain; Piriformis syndrome; Trigger point injection.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures

References
-
- Kuan TS. Current studies on myofascial pain syndrome. Curr Pain Headache Rep 2009;13(5):365–9. - PubMed
-
- Shah JP, Phillips TM, Danoff JV, et al. An in vivo microanalytical technique for measuring the local biochemical milieu of human skeletal muscle. J Appl Physiol (1985) 2005;99(5):1977–84. - PubMed
-
- Gerwin RD, Dommerholt J, Shah JP. An expansion of Simons’ integrated hypothesis of trigger point formation. Curr Pain Headache Rep 2004;8(6):468–75. - PubMed
-
- Fernández-de-las-Peñas C, Cuadrado ML, Arendt-Nielsen L, et al. Myofascial trigger points and sensitization: an updated pain model for tension-type headache. Cephalalgia 2007;27(5):383–93. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
