

FLAMES with Elevated Myelin Basic Protein Followed by Myelitis
- PMID: 35527028
- PMCID: PMC9790785
- DOI: 10.2169/internalmedicine.9439-22
FLAMES with Elevated Myelin Basic Protein Followed by Myelitis
Abstract
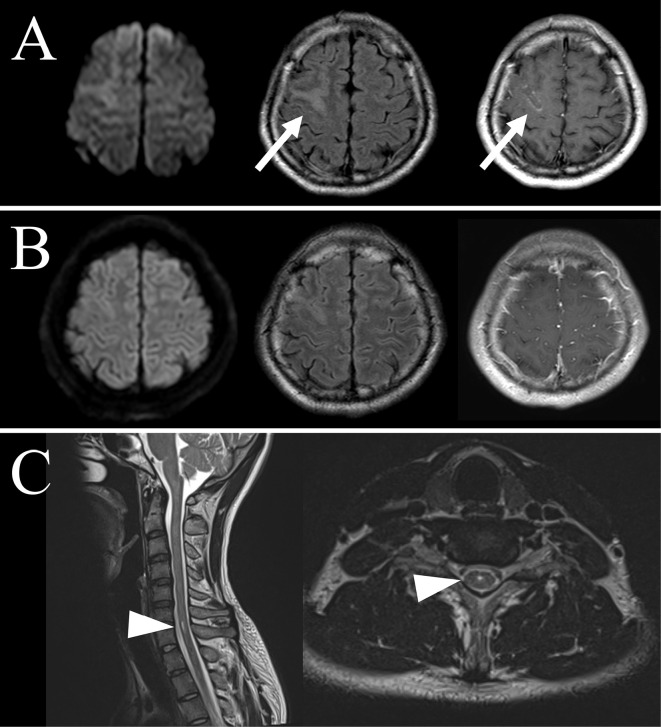
The pathophysiology of unilateral cortical fluid-attenuated inversion recovery (FLAIR)-hyperintense lesions in anti-myelin oligodendrocyte glycoprotein (MOG)-associated encephalitis with seizures (FLAMES) is unclear. A 26-year-old man was referred because of a seizure. FLAIR showed an increased signal intensity and swelling of the right frontal cortex. His symptoms and imaging abnormalities were improved after intravenous methylprednisolone therapy. MOG antibody was detected both in serum and cerebrospinal fluid (CSF). Therefore, the patient was diagnosed with FLAMES. Myelin basic protein (MBP) was elevated in CSF. The high MBP value in the CSF in the present case suggested that demyelination as well as inflammation can occur in some FLAMES patients.
Keywords: encephalitis; myelin basic protein; myelin oligodendrocyte glycoprotein antibody; myelitis; seizure.
Conflict of interest statement
Figures
References
-
- Budhram A, Mirian A, Le C, Hosseini-Moghaddam SM, Sharma M, Nicolle MW. Unilateral cortical FLAIR-hyperintense lesions in anti-MOG-associated encephalitis with seizures (FLAMES): characterization of a distinct clinico-radiographic syndrome. J Neurol 266: 2481-2487, 2019. - PubMed
-
- Numa S, Kasai T, Kondo T, et al. . An adult case of anti-myelin oligodendrocyte glycoprotein (MOG) antibody-associated multiphasic acute disseminated encephalomyelitis at 33-year intervals. Intern Med 55: 699-702, 2016. - PubMed
-
- Yamamoto D, Uchiyama T, Ohashi T, Iizuka T. Case of steroid-responsive unilateral encephalitis with anti-myelin oligodendrocyte glycoprotein antibodies. Neurol Clin Neurosci 5: 101-102, 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous