

Neutrophil Infiltration and Acinar-ductal Metaplasia Are the Main Pathological Findings in Pembrolizumab-induced Pancreatitis
- PMID: 35527030
- PMCID: PMC9841103
- DOI: 10.2169/internalmedicine.9565-22
Neutrophil Infiltration and Acinar-ductal Metaplasia Are the Main Pathological Findings in Pembrolizumab-induced Pancreatitis
Abstract
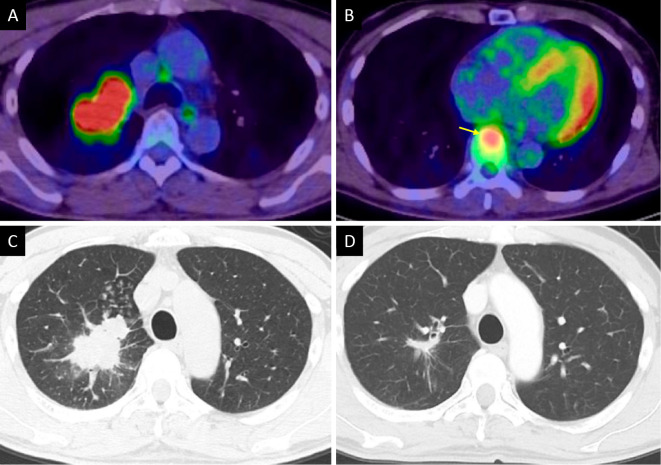
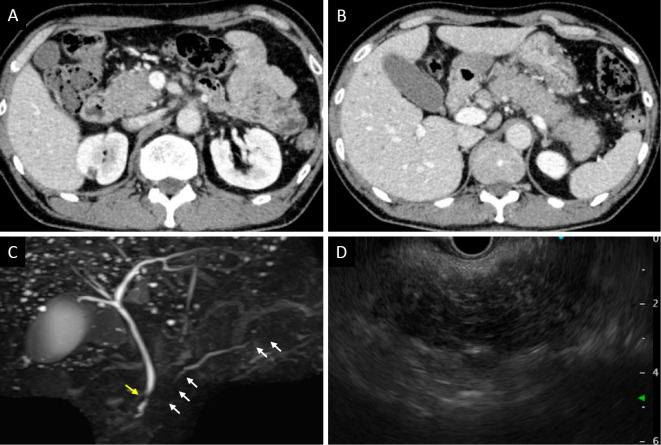
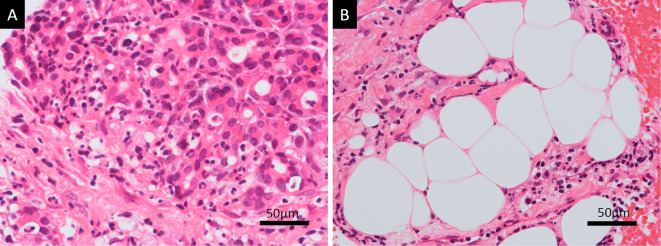
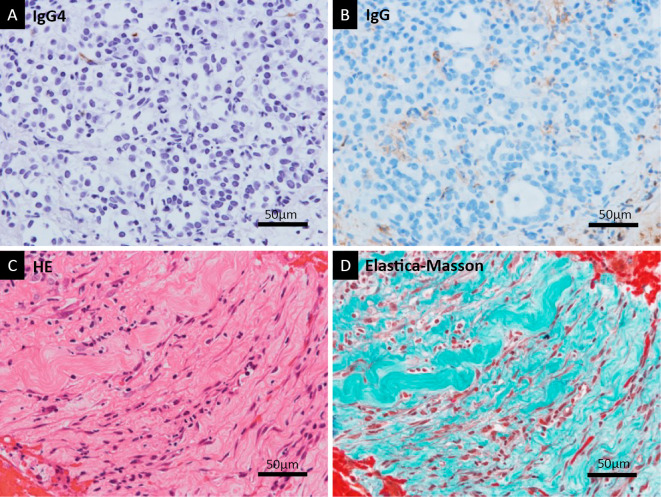
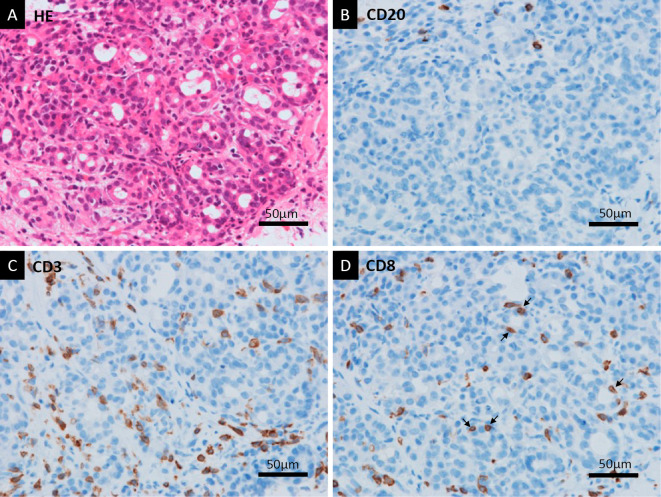
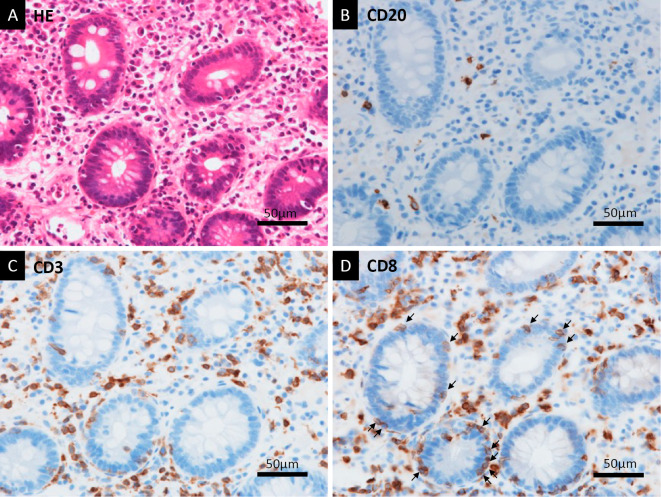
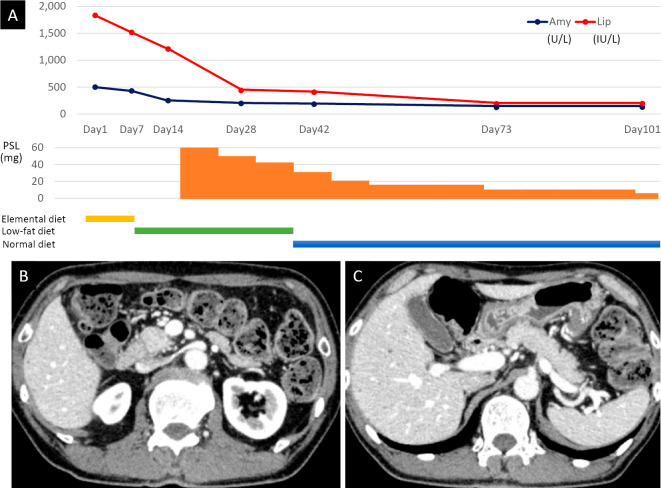
The histopathological findings of immune checkpoint inhibitor (ICI)-induced pancreatitis have rarely been reported. A 56-year-old man with squamous cell carcinoma of the lung with bone metastasis was being treated with pembrolizumab, an anti-programmed cell death protein-1 antibody. After 13 doses, he was referred to our department due to pancreatitis. Despite characteristic symptoms of acute pancreatitis, imaging findings were similar to those of autoimmune pancreatitis. However, a histological examination showed neutrophil-based inflammatory cell infiltration and acinar-ductal metaplasia. Immunostaining showed CD8-positive T lymphocyte infiltration. This case revealed the characteristic histopathology of pembrolizumab-induced pancreatitis, which was previously poorly understood.
Keywords: adverse drug event; endoscopic ultrasonography; immune checkpoint inhibitor; immunohistochemistry; pancreatitis; pembrolizumab.
Conflict of interest statement
Figures
References
-
- La-Beck NM, Jean GW, Huynh C, Alzghari SK, Lowe DB. Immune checkpoint inhibitors: new insight and current place in cancer therapy. Pharmacotherapy 35: 963-976, 2015. - PubMed
-
- Hofmann L, Forschner A, Loquai C, et al. . Cutaneous, gastrointestinal, hepatic, endocrine, and renal side-effect of anti-PD-1 therapy. Eur J Cancer 60: 190-209, 2016. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials