

Identifying opportunities for pediatric medication therapy management in children with medical complexity
- PMID: 35527209
- PMCID: PMC9464681
- DOI: 10.1016/j.japh.2022.04.005
Identifying opportunities for pediatric medication therapy management in children with medical complexity
Abstract
Background: Despite potential benefits of medication therapy management (MTM) for complex pediatric patients, implementation of pediatric MTM services is rare.
Objectives: To describe how a standardized pediatric MTM model identifies potential interventions and their impact on medication regimen complexity index (MRCI) scores in children with medical complexity (CMC) and polypharmacy.
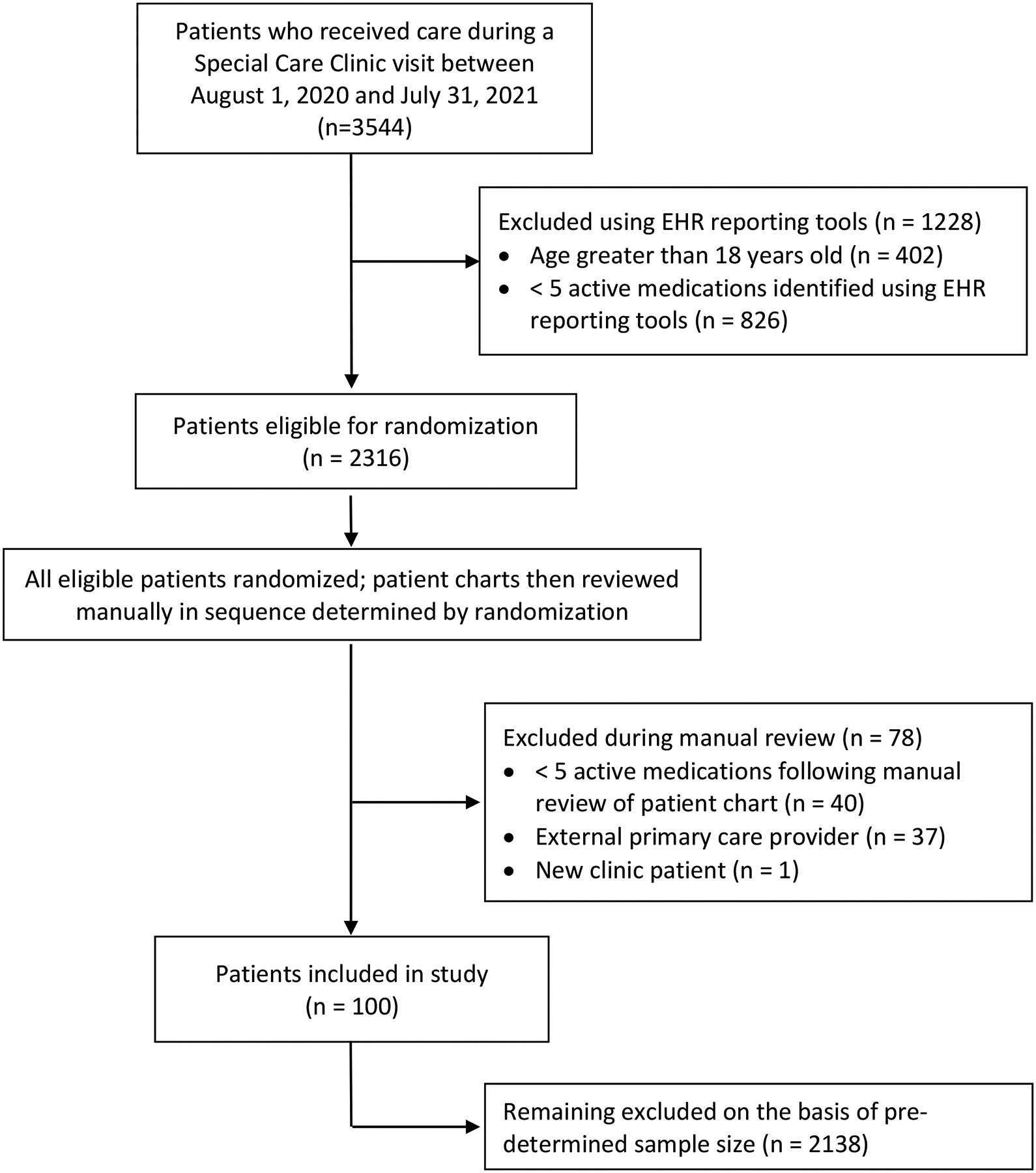
Methods: This retrospective proof-of-concept study included pediatric patients receiving primary care in a large outpatient primary care medical home for CMC within a tertiary freestanding children's hospital from August 2020 to July 2021. Medication profiles of established patients aged 0-18 years with at least 5 active medications at the time of the index visit were assessed for medication-related concerns, potential interventions, and potential impact of proposed interventions on MRCI scores.
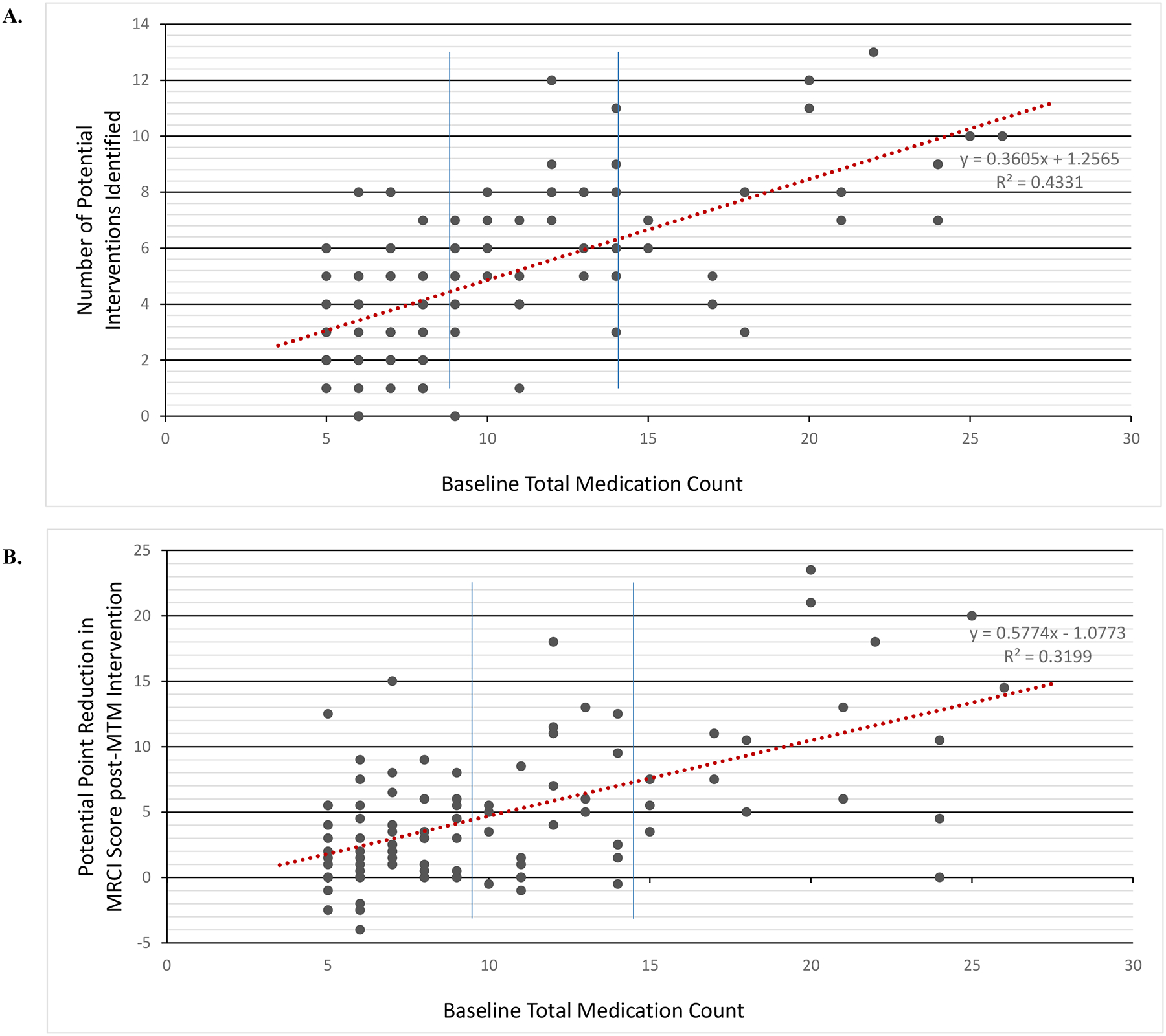
Results: Among 100 patients, an average of 3.4 ± 2.6 medication-related concerns was identified using the pediatric MTM model. Common medication-related concerns (>25% of patients) included inappropriate or unnecessary therapy, suboptimal therapy, undertreated symptom, adverse effect, clinically impactful drug-drug interaction, or duplication of therapy. A total of 97% had opportunities for 5.0 ± 2.9 potential interventions. Most common proposed interventions included drug discontinuation trial (69%), patient or caregiver education (55%), dosage form modification (51%), dose modification (49%), and frequency modification (46%). The mean baseline MRCI score was 32.6 (95% CI 29.3-35.8) among all patients. MRCI scores decreased by a mean of 4.9 (95% CI 3.8-5.9) after application of the theoretical interventions (P < 0.001). Mean potential score reduction was not significantly affected by patient age or number of complex chronic conditions. Potential impact of the proposed interventions on MRCI score was significantly greater in patients with higher baseline medication counts (P < 0.001).
Conclusion: Most CMC would likely benefit from a pharmacist-guided pediatric MTM service. A standardized review of active medication regimens identified multiple medication-related concerns and potential interventions for nearly all patients. Proposed medication interventions would significantly reduce medication regimen complexity as measured by MRCI. Further prospective evaluation of a pharmacist-guided pediatric MTM service is warranted.
Copyright © 2022 American Pharmacists Association®. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
A coordinated approach for managing polypharmacy among children with medical complexity: rationale and design of the Pediatric Medication Therapy Management (pMTM) randomized controlled trial.BMC Health Serv Res. 2023 Apr 29;23(1):414. doi: 10.1186/s12913-023-09439-y. BMC Health Serv Res. 2023. PMID: 37120509 Free PMC article. Clinical Trial.
-
Validation of a patient-level medication regimen complexity index as a possible tool to identify patients for medication therapy management intervention.Pharmacotherapy. 2014 Aug;34(8):826-35. doi: 10.1002/phar.1452. Epub 2014 Jun 20. Pharmacotherapy. 2014. PMID: 24947636 Free PMC article.
-
Looking beyond polypharmacy: quantification of medication regimen complexity in the elderly.Am J Geriatr Pharmacother. 2012 Aug;10(4):223-9. doi: 10.1016/j.amjopharm.2012.06.002. Epub 2012 Jun 29. Am J Geriatr Pharmacother. 2012. PMID: 22749668
-
Medication Regimen Complexity Index in the Elderly in an Outpatient Setting: A Literature Review.Consult Pharm. 2018 Sep 1;33(9):484-496. doi: 10.4140/TCP.n.2018.484. Consult Pharm. 2018. PMID: 30185289 Review.
-
Integrating medication therapy management in the primary care medical home: A review of randomized controlled trials.Am J Health Syst Pharm. 2011 Feb 15;68(4):335-45. doi: 10.2146/ajhp100405. Am J Health Syst Pharm. 2011. PMID: 21289329 Review.
Cited by
-
Drug-Drug Interactions Involving High-Alert Medications that Lead to Interaction-Associated Symptoms in Pediatric Intensive Care Patients: A Retrospective Study.Paediatr Drugs. 2024 Sep;26(5):619-629. doi: 10.1007/s40272-024-00641-x. Epub 2024 Jul 4. Paediatr Drugs. 2024. PMID: 38963501 Free PMC article.
-
Polypharmacy-An Important Contributor to Health and Safety for Children With Medical Complexity: How Can We Improve Care for This Vulnerable Population?J Pediatr Pharmacol Ther. 2024 Apr;29(2):96-99. doi: 10.5863/1551-6776-29.2.96. Epub 2024 Apr 8. J Pediatr Pharmacol Ther. 2024. PMID: 38596412 Free PMC article. No abstract available.
-
Challenges of managing pediatric polypharmacy in a pediatric complex care program: A qualitative pilot study.J Am Pharm Assoc (2003). 2025 Jul-Aug;65(4):102391. doi: 10.1016/j.japh.2025.102391. Epub 2025 Mar 22. J Am Pharm Assoc (2003). 2025. PMID: 40127839
-
Making Polypharmacy Safer for Children with Medical Complexity.J Pediatr. 2023 Mar;254:4-10. doi: 10.1016/j.jpeds.2022.10.012. Epub 2022 Oct 15. J Pediatr. 2023. PMID: 36252865 Free PMC article.
-
Annual Medication Use and Costs Among Children.JAMA Netw Open. 2025 Mar 3;8(3):e251529. doi: 10.1001/jamanetworkopen.2025.1529. JAMA Netw Open. 2025. PMID: 40126482 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
