

Association between annual change in FEV1 and comorbidities or impulse oscillometry in chronic obstructive pulmonary disease
- PMID: 35527263
- PMCID: PMC9080138
- DOI: 10.1186/s12890-022-01980-6
Association between annual change in FEV1 and comorbidities or impulse oscillometry in chronic obstructive pulmonary disease
Abstract
Background: Chronic obstructive pulmonary disease (COPD) is characterized by persistent respiratory symptoms and airflow limitation. The decline in forced expiratory volume in one second (FEV1) is considered to be one of the most important outcome measures for evaluating disease progression. However, the only intervention proven to improve COPD prognosis is smoking cessation. This study therefore investigated the factors associated with annual FEV1 decline in COPD.
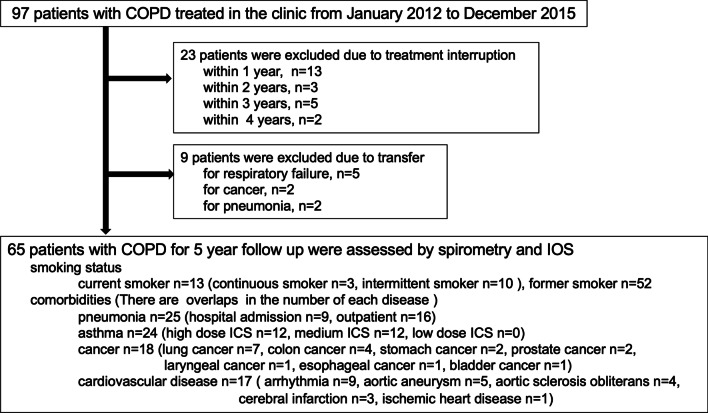
Methods: This retrospective study followed up 65 patients treated for COPD for 5 years: 13 current smokers and 52 former smokers, 25 with pneumonia, 24 with asthma, 18 with cancer, and 17 with cardiovascular disease. The patients were divided into groups based on clinical cutoff parameters of the impulse oscillometry system (IOS): 11 high and 54 low R5, 8 high and 57 low R20, 21 high and 44 low R5-R20, 26 high and 39 low X5, 38 high and 27 low Fres, and 36 high and 29 low AX. We investigated whether the decline in FEV1 was associated with comorbidities and IOS parameters.
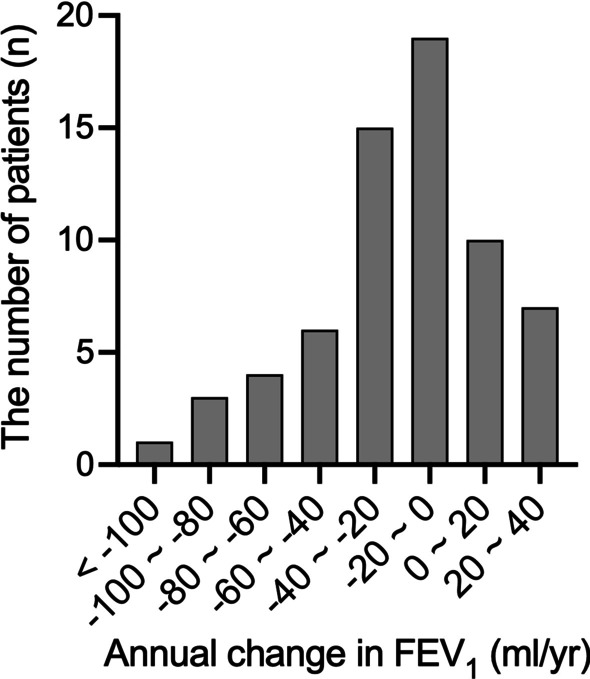
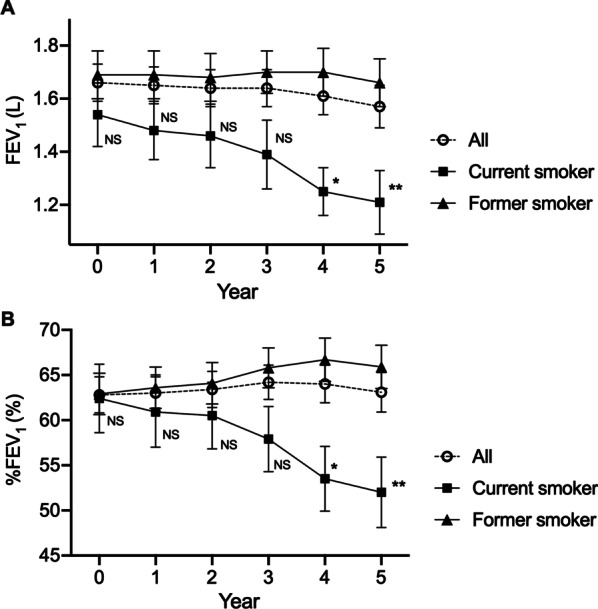
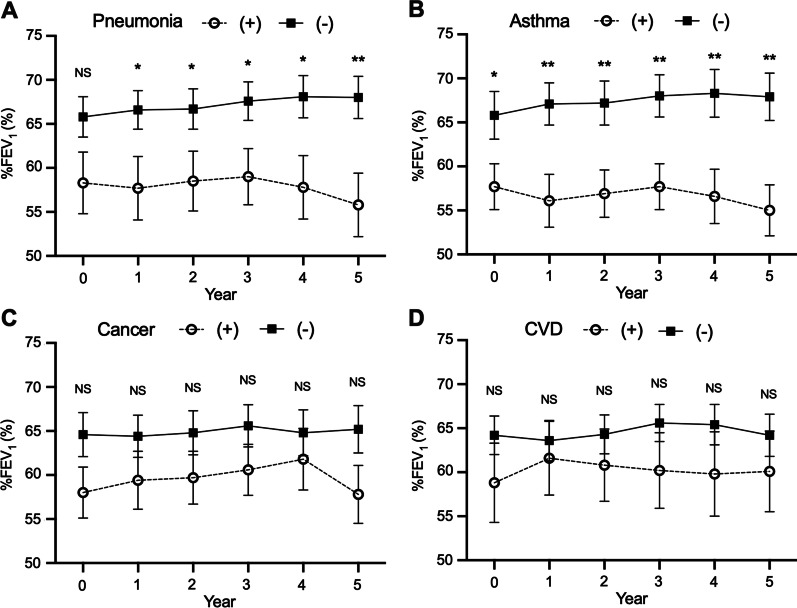
Results: The annual change in FEV1 over 5 years was significantly affected by smoking status (current - 66.2 mL/year vs. former - 5.7 mL/year, p < 0.01), pneumonia (with - 31.5 mL/year vs. without - 8.9 mL/year, p < 0.05), asthma (with - 30.2 mL/year vs. - 10.8 mL/year, p < 0.01), but not by cancer and cardiovascular disease. In the groups defined by IOS results, only the high AX group had significantly more annual decline in FEV1 and %FEV1 than the low AX group (- 22.1 vs. - 12.8, p < 0.05 and - 0.20 vs. 0.40, p < 0.05, respectively).
Conclusions: Continuing smoking as well as complications in pneumonia and asthma would be risk factors for the progression of COPD. AX might be a suitable parameter to predict the prognosis of patients with COPD.
Keywords: COPD Assessment Test; Chronic obstructive pulmonary disease; Impulse oscillometry system; Pulmonary function test; St. George’s Respiratory Questionnaire.
© 2022. The Author(s).
Conflict of interest statement
None of the authors have a conflict of interest to declare.
Figures
References
-
- Global initiative for chronic obstructive lung disease. Global strategy for diagnosis, management, and prevention of chronic obstructive pulmonary disease 2021. Available from: https://goldcopd.org/.
-
- Celli BR, Thomas NE, Anderson JA, Ferguson GT, Jenkins CR, Jones PW, Vestbo J, Knobil K, Yates JC, Calverley PM. Effect of pharmacotherapy on rate of decline of lung function in chronic obstructive pulmonary disease: results from the TORCH study. Am J Respir Crit Care Med. 2008;178:332–338. doi: 10.1164/rccm.200712-1869OC. - DOI - PubMed
-
- Vestbo J, Edwards LD, Scanlon PD, Yates JC, Agusti A, Bakke P, Calverley PM, Celli B, Coxson HO, Crim C, Lomas DA, MacNee W, Miller BE, Silverman EK, Tal-Singer R, Wouters E, Rennard SI, Investigators E. Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med. 2011;365:1184–1192. doi: 10.1056/NEJMoa1105482. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
