

The true costs of cesarean delivery for patients in rural Rwanda: Accounting for post-discharge expenses in estimated health expenditures
- PMID: 35527274
- PMCID: PMC9080175
- DOI: 10.1186/s12939-022-01664-x
The true costs of cesarean delivery for patients in rural Rwanda: Accounting for post-discharge expenses in estimated health expenditures
Abstract
Introduction: While it is recognized that there are costs associated with postoperative patient follow-up, risk assessments of catastrophic health expenditures (CHEs) due to surgery in sub-Saharan Africa rarely include expenses after discharge. We describe patient-level costs for cesarean section (c-section) and follow-up care up to postoperative day (POD) 30 and evaluate the contribution of follow-up to CHEs in rural Rwanda.
Methods: We interviewed women who delivered via c-section at Kirehe District Hospital between September 2019 and February 2020. Expenditure details were captured on an adapted surgical indicator financial survey tool and extracted from the hospital billing system. CHE was defined as health expenditure of ≥ 10% of annual household expenditure. We report the cost of c-section up to 30 days after discharge, the rate of CHE among c-section patients stratified by in-hospital costs and post-discharge follow-up costs, and the main contributors to c-section follow-up costs. We performed a multivariate logistic regression using a backward stepwise process to determine independent predictors of CHE at POD30 at α ≤ 0.05.
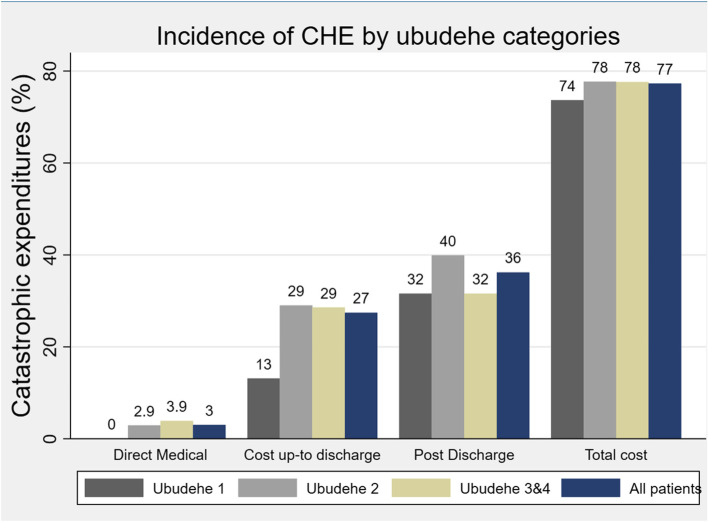
Results: Of the 479 participants in this study, 90% were classified as impoverished before surgery and an additional 6.4% were impoverished by the c-section. The median out-of-pocket costs up to POD30 was US$122.16 (IQR: $102.94, $148.11); 63% of these expenditures were attributed to post-discharge expenses or lost opportunity costs (US$77.50; IQR: $67.70, $95.60). To afford c-section care, 64.4% borrowed money and 18.4% sold possessions. The CHE rate was 27% when only considering direct and indirect costs up to the time of discharge and 77% when including the reported expenses up to POD30. Transportation and lost household wages were the largest contributors to post-discharge costs. Further, CHE at POD30 was independently predicted by membership in community-based health insurance (aOR = 3.40, 95% CI: 1.21,9.60), being a farmer (aOR = 2.25, 95% CI:1.00,3.03), primary school education (aOR = 2.35, 95% CI:1.91,4.66), and small household sizes had 0.22 lower odds of experiencing CHE compared to large households (aOR = 0.78, 95% CI:0.66,0.91).
Conclusion: Costs associated with surgical follow-up are often neglected in financial risk calculations but contribute significantly to the risk of CHE in rural Rwanda. Insurance coverage for direct medical costs is insufficient to protect against CHE. Innovative follow-up solutions to reduce costs of patient transport and compensate for household lost wages need to be considered.
Keywords: Catastrophic health expenditure; Cesarean; Cost of post-operative care; Follow-up care; Health insurance; Healthcare access; Healthcare cost; Poverty; Rural; c-section.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests associated with this study.
Figures
Similar articles
-
Does community-based health insurance protect women from financial catastrophe after cesarean section? A prospective study from a rural hospital in Rwanda.BMC Health Serv Res. 2022 May 31;22(1):717. doi: 10.1186/s12913-022-08101-3. BMC Health Serv Res. 2022. PMID: 35642031 Free PMC article. Clinical Trial.
-
Enablers and barriers to post-discharge follow-up among women who have undergone a caesarean section: experiences from a prospective cohort in rural Rwanda.BMC Health Serv Res. 2022 Jun 2;22(1):733. doi: 10.1186/s12913-022-08137-5. BMC Health Serv Res. 2022. PMID: 35655212 Free PMC article.
-
Late and Persistent Symptoms Suggestive of Surgical Site Infections After Cesarean Section: Results from a Prospective Cohort Study in Rural Rwanda.Surg Infect (Larchmt). 2023 Dec;24(10):916-923. doi: 10.1089/sur.2023.100. Epub 2023 Nov 29. Surg Infect (Larchmt). 2023. PMID: 38032658 Free PMC article.
-
Challenges in healthcare financing for surgery in sub-Saharan Africa.Pan Afr Med J. 2021 Feb 22;38:198. doi: 10.11604/pamj.2021.38.198.27115. eCollection 2021. Pan Afr Med J. 2021. PMID: 33995804 Free PMC article. Review.
-
A review of the incidence and determinants of catastrophic health expenditure in Nigeria: Implications for universal health coverage.Int J Health Plann Manage. 2019 Oct;34(4):e1387-e1404. doi: 10.1002/hpm.2847. Epub 2019 Jul 16. Int J Health Plann Manage. 2019. PMID: 31311065 Review.
Cited by
-
Prevalence and Factors Associated With Cesarean Section Delivery among Pregnant Women Attending Rwamagana Level Two Teaching Hospital, Rwanda.Rwanda J Med Health Sci. 2024 Nov 30;7(3):435-444. doi: 10.4314/rjmhs.v7i3.5. eCollection 2024 Nov. Rwanda J Med Health Sci. 2024. PMID: 40567462 Free PMC article.
-
Commonalities and differences in injured patient experiences of accessing and receiving quality injury care: a qualitative study in three sub-Saharan African countries.BMJ Open. 2024 Jul 1;14(7):e082098. doi: 10.1136/bmjopen-2023-082098. BMJ Open. 2024. PMID: 38955369 Free PMC article.
-
Determinants of cesarean mode of childbirth among Rwandan women of childbearing age: Evidence from the 2019-2020 Rwanda Demographic and Health Survey (RDHS).Public Health Chall. 2024 Jan 30;3(1):e150. doi: 10.1002/puh2.150. eCollection 2024 Mar. Public Health Chall. 2024. PMID: 40497075 Free PMC article.
-
Patients' experiences undergoing breast evaluation in Rwanda's Women's Cancer Early Detection Program.Breast Cancer Res Treat. 2023 Dec;202(3):541-550. doi: 10.1007/s10549-023-07076-x. Epub 2023 Aug 30. Breast Cancer Res Treat. 2023. PMID: 37646967 Free PMC article.
-
Functional recovery after cesarean delivery: a prospective cohort study in rural Rwanda.BMC Pregnancy Childbirth. 2023 Dec 13;23(1):858. doi: 10.1186/s12884-023-06159-3. BMC Pregnancy Childbirth. 2023. PMID: 38087238 Free PMC article.
References
-
- Boatin AA, Schlotheuber A, Betran AP, Moller AB, Barros AJD, Boerma T, et al. Within country inequalities in caesarean section rates: Observational study of 72 low and middle income countries. BMJ. 2018;360:k55. https://pubmed.ncbi.nlm.nih.gov/29367432/. - PMC - PubMed
-
- Irani M, Deering S. Challenges affecting access to cesarean delivery and strategies to overcome them in low-income countries. Int J Gynaecol Obstet Off organ Int Fed Gynaecol Obstet. United States. 2015;131:30–4. - PubMed
-
- Ushie BA, Udoh EE, Ajayi AI. Examining inequalities in access to delivery by caesarean section in Nigeria. PLoS One. Public Library of Science. 2019;14:e0221778–e0221778. https://pubmed.ncbi.nlm.nih.gov/31465505. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
