

Socioeconomic Factors Associated With Glycemic Measurement and Poor HbA1c Control in People With Type 2 Diabetes: The Global DISCOVER Study
- PMID: 35527995
- PMCID: PMC9072655
- DOI: 10.3389/fendo.2022.831676
Socioeconomic Factors Associated With Glycemic Measurement and Poor HbA1c Control in People With Type 2 Diabetes: The Global DISCOVER Study
Abstract
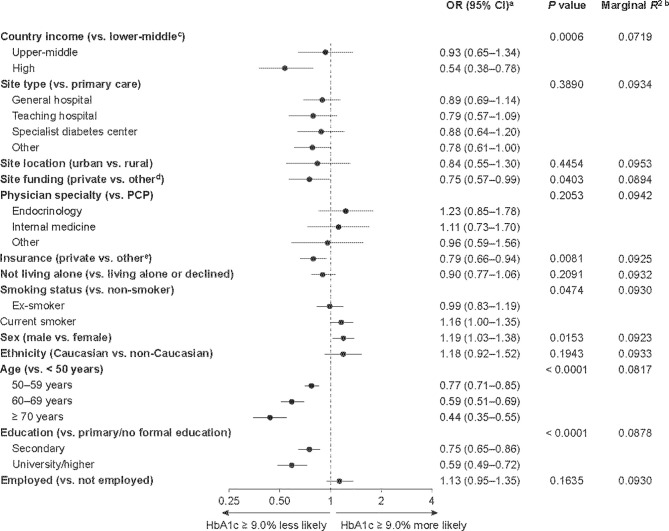
DISCOVER is a 3-year observational study program of 15,983 people with type 2 diabetes initiating second-line glucose-lowering therapy in 38 countries. We investigated the association between socioeconomic status and both the availability of a baseline glycated hemoglobin (HbA1c) measurement and poor glycemic control (HbA1c level ≥ 9.0%) in participants enrolled in DISCOVER. Factors associated with a lack of baseline HbA1c measurement or an HbA1c level ≥ 9.0% were assessed using three-level hierarchical logistic models. Overall, 19.1% of participants did not have a baseline HbA1c measurement recorded. Lower-middle country income (vs. high) and primary/no formal education (vs. university education) were independently associated with a reduced likelihood of having a baseline HbA1c measurement (odds ratio [95% confidence interval]: 0.11 [0.03-0.49] and 0.81 [0.66-0.98], respectively. Of the participants with an available HbA1c measurement, 26.9% had an HbA1c level ≥ 9.0%; 68.7% of these individuals were from lower- or upper-middle-income countries. Factors associated with an increased likelihood of poor glycemic control included low country income, treatment at a site with public and/or governmental funding (vs. private funding) and having public or no health insurance (vs. private). A substantial proportion of DISCOVER participants did not have an HbA1c measurement; more than one-quarter of these participants had poorly controlled type 2 diabetes. Both individual- and country-level socioeconomic factors are associated with the quality of care regarding glycemic control. Awareness of these factors could help improve the management of patients with type 2 diabetes.
Keywords: glucose-lowering drug; glycemic control; observational study; socioeconomic factors; type 2 diabetes.
Copyright © 2022 Gomes, Tang, Chen, Cid-Ruzafa, Fenici, Khunti, Rathmann, Shestakova, Surmont, Watada, Medina, Shimomura, Saraiva, Cooper and Nicolucci.
Conflict of interest statement
MG, KK, WR, MS, HW, IS and AN are members of the DISCOVER Scientific Committee and received support from AstraZeneca to attend DISCOVER planning and update meetings. HC, PF, FS, JM, GS and AC are employees of AstraZeneca. JC-R is an employee of Evidera. FT is an employee of Saint Luke’s Mid America Heart Institute, which has received funding from AstraZeneca. In addition, MG has received honoraria from Merck-Serono; KK has received honoraria from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck Sharp & Dohme, Novartis, Novo Nordisk, Sanofi, Takeda, Servier and Pfizer, research support from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novartis, Novo Nordisk, Sanofi and Pfizer, and also acknowledges support from the National Institute for Health Research Applied Research Collaboration–East Midlands and the Leicester Biomedical Research Centre; WR has received research support from Novo Nordisk; MS has received honoraria from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharpe & Dohme, Novo Nordisk, Sanofi and Servier, and research support from Novo Nordisk, Sanofi and Servier; HW has received honoraria from Astellas Pharma, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Sumitomo Dainippon Pharma, Eli Lilly, Kissei Pharmaceutical, Kowa Pharmaceuticals America Inc., Kyowa Hakko Kirin, Merck Sharp & Dohme, Mitsubishi Tanabe Pharma, Novartis, Novo Nordisk, Ono Pharmaceutical, Sanofi, Sanwa Kagaku Kenkyusho and Takeda, and research support from Abbott, Astellas Pharma, AstraZeneca, Bayer, Benefit One Health Care, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Dainippon Sumitomo Pharma, Eli Lilly, Johnson & Johnson, Kissei Pharmaceutical, Kowa Pharmaceuticals America Inc., Kyowa Hakko Kirin, Merck Sharp & Dohme, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, Nitto Boseki, Novartis, Novo Nordisk, Ono Pharmaceutical, Pfizer, Sanofi, Sanwa Kagaku Kenkyusho, Taisho Toyama Pharmaceutical, Takeda and Terumo Corp; IS has received honoraria from Astellas Pharma, AstraZeneca, Boehringer Ingelheim, Kowa Pharmaceuticals America Inc., Merck Sharp & Dohme, Mitsubishi Tanabe Pharma, Novo Nordisk, Ono Pharmaceutical, Sanwa Kagaku Kenkyusho and Takeda, and research support from Astellas Pharma, AstraZeneca, Daiichi Sankyo, Eli Lilly, Japan Foundation for Applied Enzymology, Japan Science and Technology Agency, Kowa Pharmaceuticals America Inc., Kyowa Hakko Kirin, Midori Health Management Centre, Mitsubishi Tanabe Pharma, Novo Nordisk, Ono Pharmaceutical, Sanofi, Suzuken Memorial Foundation and Takeda; AN has received honoraria from AstraZeneca, Eli Lilly, Medtronic and Novo Nordisk, and research support from Artsana, Dexcom, Novo Nordisk and Sanofi. Authors HC, PF, FS, JM, GLS and AC were employed by the company AstraZeneca. FT is an employee of Saint Luke’s Mid America Heart Institute, which has received funding from AstraZeneca.The authors declare that this study received funding from AstraZeneca. The funder had the following involvement with the study: AstraZeneca designed the DISCOVER study with input and guidance from DISCOVER Scientific Committee members. An AstraZeneca team reviewed this manuscript for scientific accuracy during its development and was allowed to make suggestions. However, the final content, analysis and interpretation of the data was determined by the authors. DISCOVER is a non‑interventional study, and no drugs were supplied or funded. Statistical analyses were conducted by the Mid America Heart Institute, Kansas City, MO, USA, and were funded by AstraZeneca. Medical writing support for this manuscript was provided by Lucy Ambrose DPhil and Steph Macdonald PhD of Oxford PharmaGenesis, Oxford, UK, and was funded by AstraZeneca.
Figures

Similar articles
-
Glycaemic control in patients with type 2 diabetes initiating second-line therapy: Results from the global DISCOVER study programme.Diabetes Obes Metab. 2020 Jan;22(1):66-78. doi: 10.1111/dom.13866. Epub 2019 Oct 1. Diabetes Obes Metab. 2020. PMID: 31468637 Free PMC article.
-
What are the factors associated with long-term glycaemic control in patients with type 2 diabetes and elevated glycated haemoglobin (≥7.0%) at initiation of second-line therapy? Results from the DISCOVER study.Diabetes Obes Metab. 2021 Oct;23(10):2336-2343. doi: 10.1111/dom.14476. Epub 2021 Aug 2. Diabetes Obes Metab. 2021. PMID: 34212481
-
Inappropriate intensification of glucose-lowering treatment in older patients with type 2 diabetes: the global DISCOVER study.BMJ Open Diabetes Res Care. 2021 May;9(1):e001585. doi: 10.1136/bmjdrc-2020-001585. BMJ Open Diabetes Res Care. 2021. PMID: 33941550 Free PMC article.
-
Evaluation of glycated albumin (GA) and GA/HbA1c ratio for diagnosis of diabetes and glycemic control: A comprehensive review.Crit Rev Clin Lab Sci. 2017 Jun;54(4):219-232. doi: 10.1080/10408363.2017.1299684. Epub 2017 Apr 10. Crit Rev Clin Lab Sci. 2017. PMID: 28393586 Review.
-
Considerations when planning and conducting large global observational studies: Experience from the DISCOVER study of patients with type 2 diabetes.Prim Care Diabetes. 2023 Oct;17(5):411-419. doi: 10.1016/j.pcd.2023.07.002. Epub 2023 Aug 5. Prim Care Diabetes. 2023. PMID: 37544790 Review.
Cited by
-
Diabetes mellitus and inequalities in the equipment and use of information technologies as a socioeconomic determinant of health in Spain.Front Public Health. 2023 Jan 9;10:1033461. doi: 10.3389/fpubh.2022.1033461. eCollection 2022. Front Public Health. 2023. PMID: 36699934 Free PMC article.
-
Exploring Inequalities in the Use, Quality, and Outcome of the Diabetes Management Program of Indonesian National Health Insurance.Health Equity. 2023 Sep 27;7(1):644-652. doi: 10.1089/heq.2023.0025. eCollection 2023. Health Equity. 2023. PMID: 37786529 Free PMC article.
-
Dietary Antioxidant Minerals (Cr, Mg, Cu, Se, Zn) in Diabetic Children and their Relationship with Fasting and Postprandial Blood Glucose.Int J Prev Med. 2025 Apr 24;16:24. doi: 10.4103/ijpvm.ijpvm_119_24. eCollection 2025. Int J Prev Med. 2025. PMID: 40376080 Free PMC article.
-
Socioeconomic Status, Modifiable Factors, and Risk of Microvascular Complications in Individuals With Type 2 Diabetes: A Cohort Study From the UK Biobank.J Diabetes. 2025 Apr;17(4):e70079. doi: 10.1111/1753-0407.70079. J Diabetes. 2025. PMID: 40171824 Free PMC article.
-
The effect of close and intensive therapeutic monitoring of patients with poorly controlled type 2 diabetes with different glycemic background.Medicine (Baltimore). 2023 Dec 15;102(50):e36680. doi: 10.1097/MD.0000000000036680. Medicine (Baltimore). 2023. PMID: 38115271 Free PMC article.
References
-
- Baker EH. Socioeconomic Status, Definition. In: Cockerham WC, Dingwall R, Quah S, editors. The Wiley Blackwell Encyclopedia of Health, Illness, Behavior, and Society. London: Oxford University Press; (2014). p. 151–65.
-
- Kyrou I, Tsigos C, Mavrogianni C, Cardon G, Van Stappen V, Latomme J, et al. . Sociodemographic and Lifestyle-Related Risk Factors for Identifying Vulnerable Groups for Type 2 Diabetes: A Narrative Review With Emphasis on Data From Europe. BMC Endocr Disord (2020) 20:134. doi: 10.1186/s12902-019-0463-3 - DOI - PMC - PubMed
-
- International Diabetes Federation, IDF . Diabetes Atlas. Available at: https://www.diabetesatlas.org (Accessed 15 May 2020).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical