

Preventing pediatric chronic postsurgical pain: Time for increased rigor
- PMID: 35528039
- PMCID: PMC9067470
- DOI: 10.1080/24740527.2021.2019576
Preventing pediatric chronic postsurgical pain: Time for increased rigor
Abstract
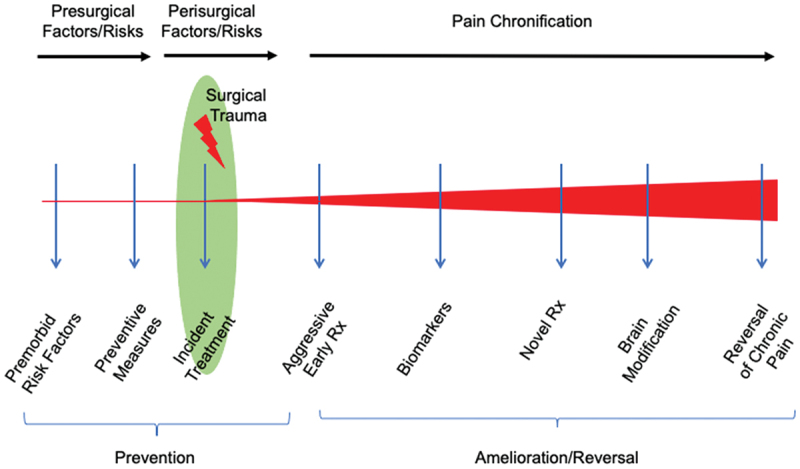
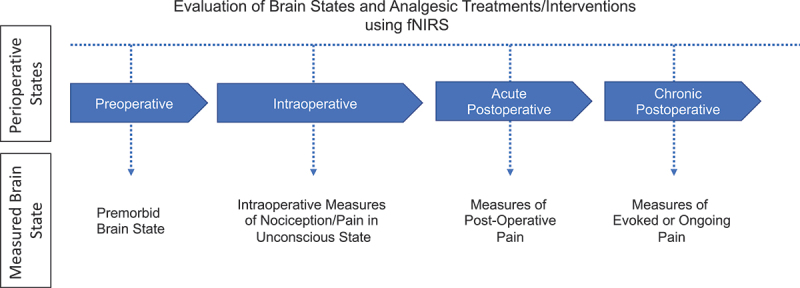
Chronic postsurgical pain (CPSP) results from a cascade of events in the peripheral and central nervous systems following surgery. Several clinical predictors, including the prior pain state, premorbid psychological state (e.g., anxiety, catastrophizing), intraoperative surgical load (establishment of peripheral and central sensitization), and acute postoperative pain management, may contribute to the patient's risk of developing CPSP. However, research on the neurobiological and biobehavioral mechanisms contributing to pediatric CPSP and effective preemptive/treatment strategies are still lacking. Here we evaluate the perisurgical process by identifying key problems and propose potential solutions for the pre-, intra-, and postoperative pain states to both prevent and manage the transition of acute to chronic pain. We propose an eight-step process involving preemptive and preventative analgesia, behavioral interventions, and the use of biomarkers (brain-based, inflammatory, or genetic) to facilitate timely evaluation and treatment of premorbid psychological factors, ongoing surgical pain, and postoperative pain to provide an overall improved outcome. By achieving this, we can begin to establish personalized precision medicine for children and adolescents presenting to surgery and subsequent treatment selection.
La douleur chronique post-chirurgicale (DCPC) résulte d'une cascade d'événements dans les systèmes nerveux central et périphérique suite à une intervention chirurgicale. Plusieurs prédicteurs cliniques, y compris l'état douloureux antérieur, l'état psychologique prémorbide (p. ex., anxiété, catastrophisme), la charge chirurgicale peropératoire (établissement d'une sensibilisation périphérique et centrale) et la prise en charge de la douleur postopératoire aiguë, peuvent contribuer au risque du patient de développer une DCPC. Cependant, la recherche sur les mécanismes neurobiologiques et biocomportementaux contribuant à la DCPC pédiatrique et sur les stratégies de prévention et de traitement efficaces font encore défaut. Nous évaluons ici le processus périchirurgical en cernant les problémes clés et en proposant des solutions potentielles pour les états douloureux pré, per et postopératoires afin de prévenir et de prendre en charge la transition de la douleur aiguë à la douleur chronique. Nous proposons un processus en huit étapes impliquant l'analgésie préemptive et préventive, les interventions comportementales et l'utilisation de biomarqueurs (cérébraux, inflammatoires ou génétiques) pour faciliter l'évaluation et le traitement opportuns des facteurs psychologiques prémorbides, de la douleur chirurgicale persistante et de la douleur postopératoire afin d'améliorer le résultat global. En y parvenant, nous pouvons commencer à établir une médecine de précision personnalisée pour les enfants et les adolescents qui subissent une intervention chirurgicale et à la sélection du traitement qui s'ensuit.
Keywords: analgesia; biomarker; chronic pain; cognitive behavioral therapy; fNIRS; opioids; postoperative pain; surgery.
© 2022 The Author(s). Published with license by Taylor & Francis Group, LLC.
Conflict of interest statement
David Borsook is a consultant for Redpin Therapeutics and Mitobridge; however, there is a no conflict of interest relevant to the content of this article. All other authors have no conflicts of interest to report.
Figures
Similar articles
-
Identifying risk factors for chronic postsurgical pain and preventive measures: a comprehensive update.Expert Rev Neurother. 2023 Jul-Dec;23(12):1297-1310. doi: 10.1080/14737175.2023.2284872. Epub 2023 Dec 15. Expert Rev Neurother. 2023. PMID: 37999989 Review.
-
Transition from Acute to Chronic Pain: Evaluating Risk for Chronic Postsurgical Pain.Pain Physician. 2019 Sep;22(5):479-488. Pain Physician. 2019. PMID: 31561647 Review.
-
A Conceptual Model of Biopsychosocial Mechanisms of Transition from Acute to Chronic Postsurgical Pain in Children and Adolescents.J Pain Res. 2020 Nov 24;13:3071-3080. doi: 10.2147/JPR.S239320. eCollection 2020. J Pain Res. 2020. PMID: 33262642 Free PMC article. Review.
-
Practical strategies for the prevention and management of chronic postsurgical pain.Korean J Pain. 2023 Apr 1;36(2):149-162. doi: 10.3344/kjp.23080. Korean J Pain. 2023. PMID: 36973967 Free PMC article. Review.
-
The role of anxiety and related states in pediatric postsurgical pain.Can J Pain. 2020 Dec 30;4(4):26-36. doi: 10.1080/24740527.2020.1847600. Can J Pain. 2020. PMID: 33987517 Free PMC article. Review.
Cited by
-
Special issue: Developmental perspectives on the transition of acute to chronic pain after surgery.Can J Pain. 2022 Jul 26;6(2):46-48. doi: 10.1080/24740527.2022.2090323. eCollection 2022. Can J Pain. 2022. PMID: 35910394 Free PMC article. No abstract available.
-
The Challenge of Managing Neuropathic Pain in Children and Adolescents with Cancer.Cancers (Basel). 2025 Jan 29;17(3):460. doi: 10.3390/cancers17030460. Cancers (Basel). 2025. PMID: 39941827 Free PMC article. Review.
-
Opioid prescription rates associated with surgery among adolescents in the United States from 2015 to 2020.Paediatr Anaesth. 2023 Dec;33(12):1083-1090. doi: 10.1111/pan.14753. Epub 2023 Oct 4. Paediatr Anaesth. 2023. PMID: 37789737 Free PMC article.
-
Exploring Comorbidities in Adolescent and Young Adults with Hypermobile Ehlers-Danlos Syndrome with and without a Surgical History: A Preliminary Investigation.Children (Basel). 2023 Sep 16;10(9):1562. doi: 10.3390/children10091562. Children (Basel). 2023. PMID: 37761523 Free PMC article.
-
Chronic Postsurgical Pain in Children and Adolescents: A Call for Action.J Pain Res. 2024 May 29;17:1967-1978. doi: 10.2147/JPR.S464009. eCollection 2024. J Pain Res. 2024. PMID: 38828088 Free PMC article. Review.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources