

Cardiac tamponade as the initial presentation of autoimmune polyglandular syndrome Type 2: a case report
- PMID: 35528129
- PMCID: PMC9071554
- DOI: 10.1093/ehjcr/ytac145
Cardiac tamponade as the initial presentation of autoimmune polyglandular syndrome Type 2: a case report
Abstract
Background: Cardiac tamponade is a rare but serious manifestation of autoimmune polyglandular syndrome Type 2 (APS 2). Patients often present with symptoms of thyroid dysfunction and adrenal insufficiency, but the insidious onset of the disease may lead to delayed diagnosis, which can progress rapidly to haemodynamic instability requiring urgent intervention.
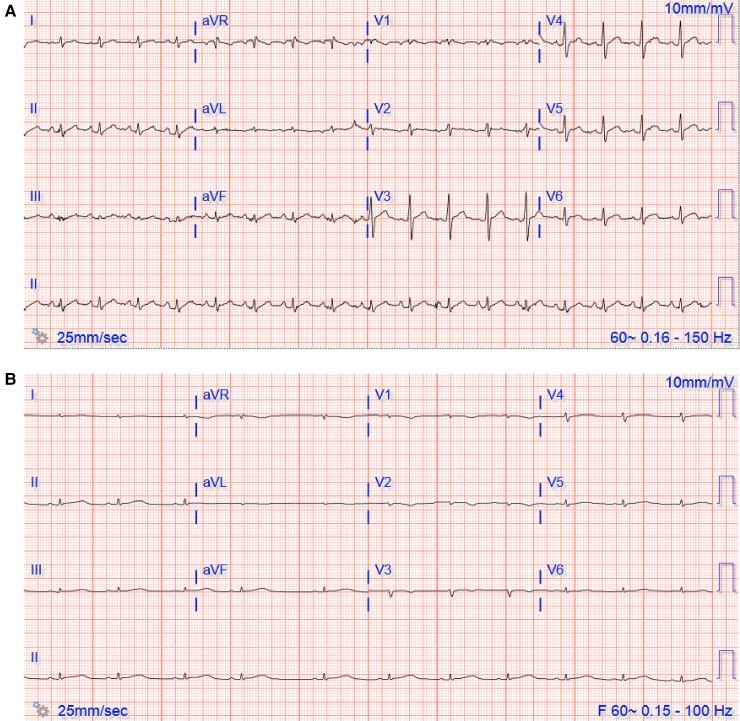
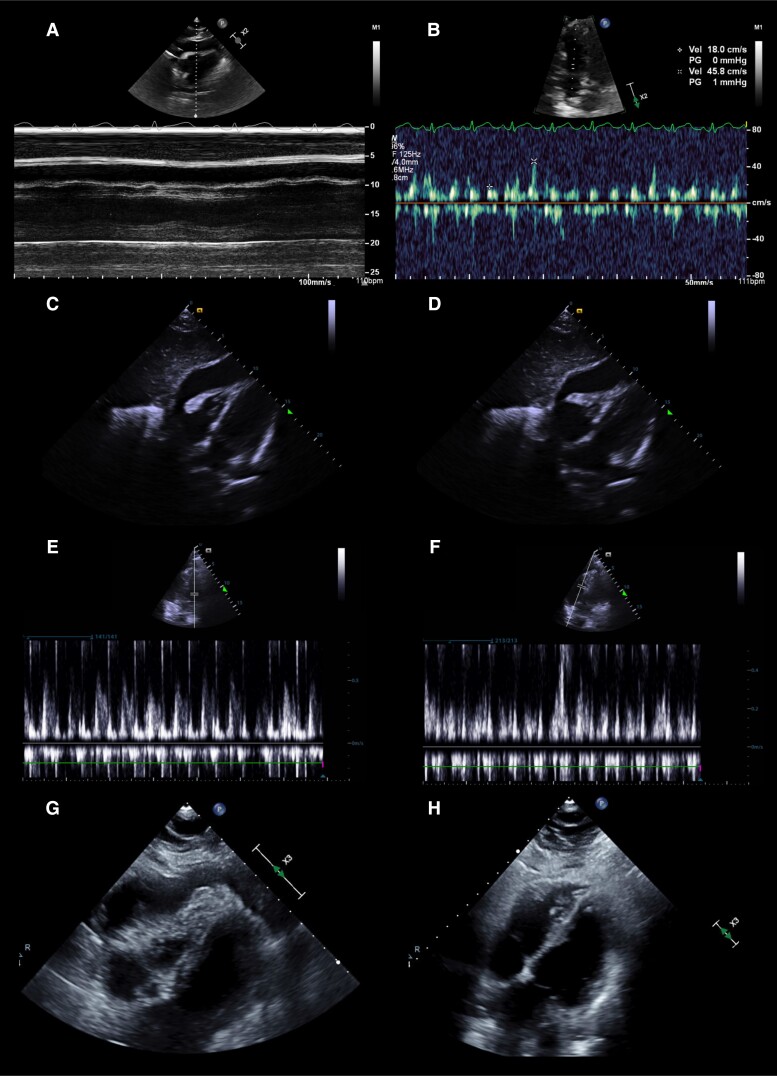
Case summary: A 39-year-old previously healthy male was admitted with cardiac tamponade complicated by cardiac arrest requiring emergent pericardiocentesis. An extensive work up revealed primary adrenal insufficiency and Hashimoto's thyroiditis. His positive autoantibodies to thyroid peroxidase and 21-hydroxylase combined with rapid improvement with initiation of corticosteroids and levothyroxine confirmed a diagnosis of APS 2.
Discussion: Although this disease is often difficult to diagnose given its vague symptoms, it should be considered in the differential diagnosis for young patients presenting with pericardial effusion or cardiac tamponade of unknown origin. Early diagnosis and management are critical and often result in rapid improvement after appropriate treatment.
Keywords: Adrenal insufficiency; Autoimmune polyglandular syndrome Type 2; Cardiac tamponade; Case report.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Figures

References
-
- Betterle C, Dal Pra C, Mantero F, Zanchetta R. Autoimmune adrenal insufficiency and autoimmune polyendocrine syndromes: autoantibodies, autoantigens, and their applicability in diagnosis and disease prediction. Endocr Rev 2002;23:327–264. - PubMed
-
- Schatz DA, Winter WE. Autoimmune polyglandular syndrome. II: clinical syndrome and treatment. Endocrinol Metab Clin North Am 2002; 31:339–352. - PubMed
-
- Neufeld M, Maclaren NK, Blizzard RM. Two types of autoimmune Addison's disease associated with different polyglandular autoimmune (PGA) syndromes. Medicine 1981;60:355–362. - PubMed
-
- Betterle C, Volpato M, Greggio AN, Presotto F. Type 2 polyglandular autoimmune disease (Schmidt's syndrome). Journal of Pediatric Endocrinology and Metabolism 1996;9:113–123. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous