

Dissecting central post-stroke pain: a controlled symptom-psychophysical characterization
- PMID: 35528229
- PMCID: PMC9070496
- DOI: 10.1093/braincomms/fcac090
Dissecting central post-stroke pain: a controlled symptom-psychophysical characterization
Abstract
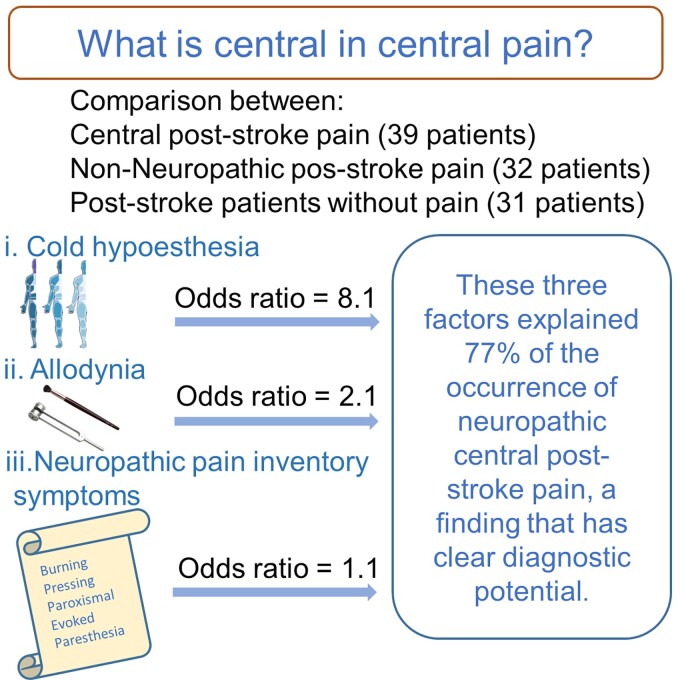
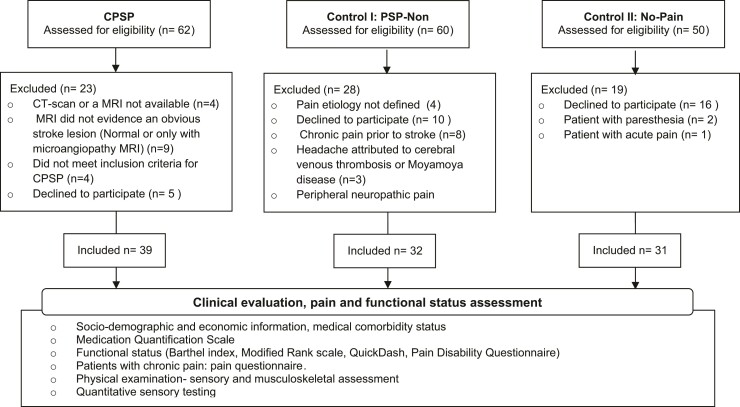
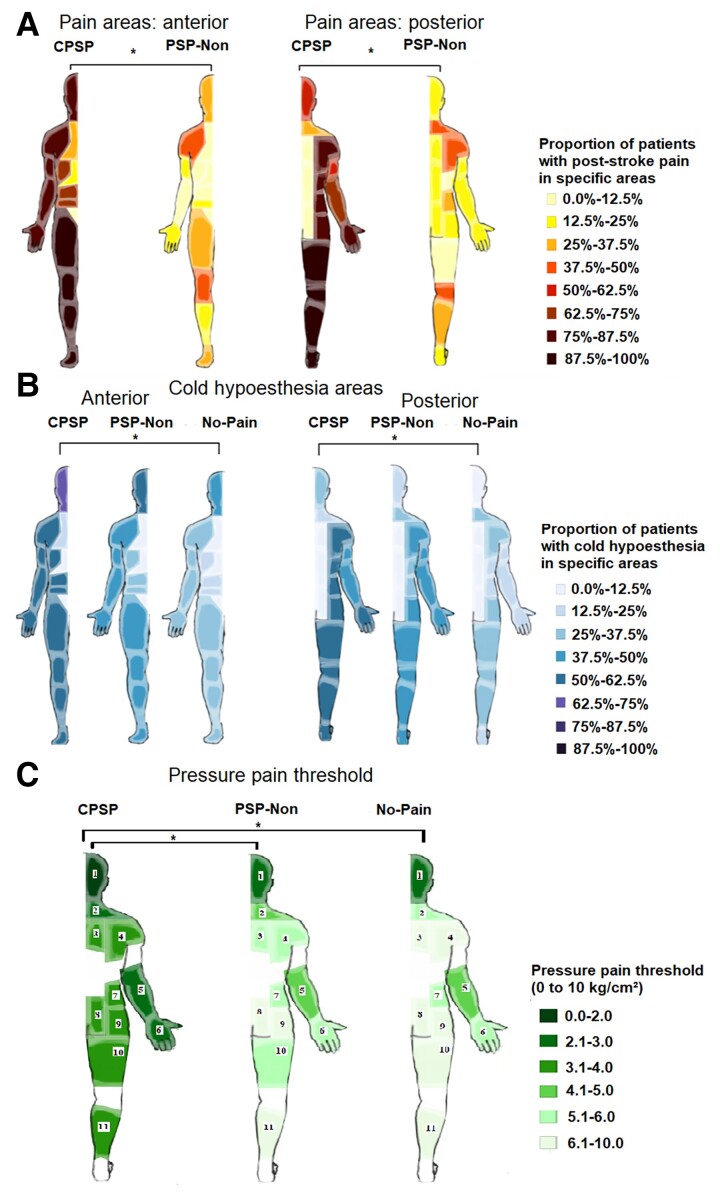
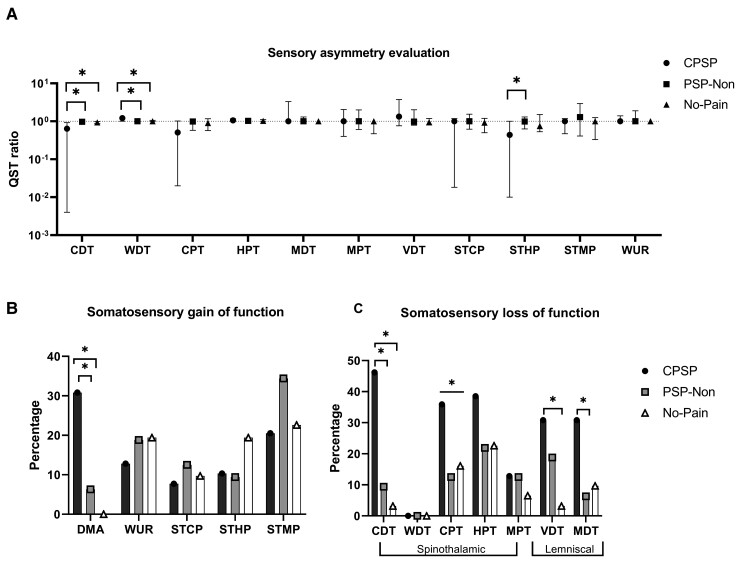
Central post-stroke pain affects up to 12% of stroke survivors and is notoriously refractory to treatment. However, stroke patients often suffer from other types of pain of non-neuropathic nature (musculoskeletal, inflammatory, complex regional) and no head-to-head comparison of their respective clinical and somatosensory profiles has been performed so far. We compared 39 patients with definite central neuropathic post-stroke pain with two matched control groups: 32 patients with exclusively non-neuropathic pain developed after stroke and 31 stroke patients not complaining of pain. Patients underwent deep phenotyping via a comprehensive assessment including clinical exam, questionnaires and quantitative sensory testing to dissect central post-stroke pain from chronic pain in general and stroke. While central post-stroke pain was mostly located in the face and limbs, non-neuropathic pain was predominantly axial and located in neck, shoulders and knees (P < 0.05). Neuropathic Pain Symptom Inventory clusters burning (82.1%, n = 32, P < 0.001), tingling (66.7%, n = 26, P < 0.001) and evoked by cold (64.1%, n = 25, P < 0.001) occurred more frequently in central post-stroke pain. Hyperpathia, thermal and mechanical allodynia also occurred more commonly in this group (P < 0.001), which also presented higher levels of deafferentation (P < 0.012) with more asymmetric cold and warm detection thresholds compared with controls. In particular, cold hypoesthesia (considered when the threshold of the affected side was <41% of the contralateral threshold) odds ratio (OR) was 12 (95% CI: 3.8-41.6) for neuropathic pain. Additionally, cold detection threshold/warm detection threshold ratio correlated with the presence of neuropathic pain (ρ = -0.4, P < 0.001). Correlations were found between specific neuropathic pain symptom clusters and quantitative sensory testing: paroxysmal pain with cold (ρ = -0.4; P = 0.008) and heat pain thresholds (ρ = 0.5; P = 0.003), burning pain with mechanical detection (ρ = -0.4; P = 0.015) and mechanical pain thresholds (ρ = -0.4, P < 0.013), evoked pain with mechanical pain threshold (ρ = -0.3; P = 0.047). Logistic regression showed that the combination of cold hypoesthesia on quantitative sensory testing, the Neuropathic Pain Symptom Inventory, and the allodynia intensity on bedside examination explained 77% of the occurrence of neuropathic pain. These findings provide insights into the clinical-psychophysics relationships in central post-stroke pain and may assist more precise distinction of neuropathic from non-neuropathic post-stroke pain in clinical practice and in future trials.
Keywords: central neuropathic pain; central post-stroke pain; neuropathic pain phenotyping; post-stroke pain; quantitative sensory testing.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Widar M, Ahlström G. Disability after a stroke and the influence of long-term pain on everyday life. Scand J Caring Sci. 2002;16(3):302–310. - PubMed
-
- Kong KH, Woon VC, Yang SY. Prevalence of chronic pain and its impact on health-related quality of life in stroke survivors. Arch Phys Med Rehabil. 2004;85(1):35–40. - PubMed
-
- Indredavik B, Rohweder G, Naalsund E, Lydersen S. Medical complications in a comprehensive stroke unit and an early supported discharge service. Stroke. 2008;39(2):414–420. - PubMed
-
- Klit H, Finnerup NB, Jensen TS. Central post-stroke pain: Clinical characteristics, pathophysiology, and management. Lancet Neurol. 2009;8(9):857–868. - PubMed
LinkOut - more resources
Full Text Sources