

Secondary Sclerosing Cholangitis in a Critically Ill Patient with Severe SARS-CoV-2 Infection: A Possibly Emergent Entity during the Current Global Pandemic
- PMID: 35528723
- PMCID: PMC9059009
- DOI: 10.1159/000521758
Secondary Sclerosing Cholangitis in a Critically Ill Patient with Severe SARS-CoV-2 Infection: A Possibly Emergent Entity during the Current Global Pandemic
Abstract
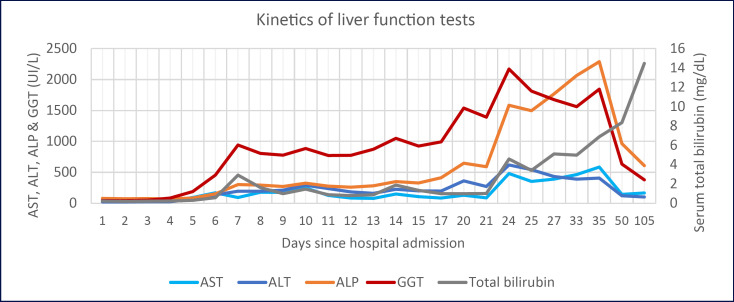
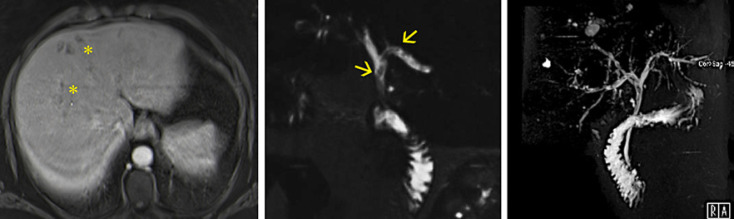
A 46-year-old woman without previous history of hepatobiliary disease was admitted to the intensive care unit due to SARS-CoV-2 infection. Admission blood tests revealed impending hyperinflammation in the context of systemic inflammatory response syndrome. She required 12 days of mechanical ventilation and vasopressor support. After admission, liver function tests became deranged in a cholestatic pattern and continued to worsen despite overall clinical improvement. Magnetic resonance cholangiopancreatography revealed liver abscesses, intrahepatic bile duct dilation with multiple strictures and some linear repletion defects at the bifurcation of the common hepatic duct. During endoscopic retrograde cholangiopancreatography, biliary casts were retrieved confirming the diagnosis of secondary sclerosing cholangitis in the critically ill patient triggered by a severe SARS-CoV-2 infection. Other causes of cholestasis and secondary sclerosing cholangitis were properly excluded. We present an illustrative case and discuss the current literature, focusing on SARS-CoV-2 infection contribution to the development of this potentially underdiagnosed and severe condition.
Uma mulher de 46 anos sem antecedentes de patologia hepatobiliar foi admitida na unidade de cuidados intensivos no contexto de infeção por SARS-CoV-2. Apresentava alterações analíticas interpretadas no contexto de síndrome de resposta inflamatória sistémica. Houve necessidade de suporte vasopressor e ventilação mecânica invasiva durante 12 dias. Após a admissão, verificou-se uma alteração das provas hepáticas com padrão colestático, com agravamento contínuo apesar da melhoria do quadro infecioso. A colangiografia por ressonância magnética revelou a presença de abcessos hepáticos, dilatação das vias biliares intrahepáticas com múltiplas estenoses e com alguns defeitos de repleção lineares na bifurcação do ducto hepático comum. Na colangiopancreatografia endoscópica retrógrada foram removidos cilindros bilares da via biliar, confirmando o diagnóstico de colangite esclerosante secundária associada aos cuidados intensivos, no contexto de uma infeção grave por SARS-CoV-2. Foram excluídas outras causas de colestase e colangite esclerosante secundária de forma exaustiva. Apresentamos um caso clínico ilustrativo com respetiva iconografia e revisão da literatura, com especial enfoque na contribuição da infeção por SARS-CoV-2 no desenvolvimento desta entidade clínica, potencialmente grave e subdiagnosticada.
Keywords: Biliary casts; COVID-19; Cholestasis; Critical care; SARS-CoV-2; Secondary sclerosing cholangitis.
Copyright © 2022 by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Secondary sclerosing cholangitis in critically ill patients: a rare disease precipitated by severe SARS-CoV-2 infection.BMJ Case Rep. 2020 Nov 9;13(11):e237984. doi: 10.1136/bcr-2020-237984. BMJ Case Rep. 2020. PMID: 33168538 Free PMC article.
-
Secondary Sclerosing Cholangitis in Critically Ill Patients: An Underdiagnosed Entity.GE Port J Gastroenterol. 2020 Feb;27(2):103-114. doi: 10.1159/000501405. Epub 2019 Jul 30. GE Port J Gastroenterol. 2020. PMID: 32266307 Free PMC article. Review.
-
Ischemic-like cholangiopathy with secondary sclerosing cholangitis in critically ill patients.Am J Gastroenterol. 2007 Jun;102(6):1221-9. doi: 10.1111/j.1572-0241.2007.01118.x. Am J Gastroenterol. 2007. PMID: 17531010
-
Biliary Cast Syndrome and Secondary Sclerosing Cholangitis in Critically Ill Patient after Long-Term Treatment in the Intensive Care Unit.Case Rep Gastroenterol. 2024 May 10;18(1):260-265. doi: 10.1159/000537957. eCollection 2024 Jan-Dec. Case Rep Gastroenterol. 2024. PMID: 38737441 Free PMC article.
-
Biliary cast formation with sclerosing cholangitis in critically ill patient: case report and literature review.Korean J Radiol. 2012 May-Jun;13(3):358-62. doi: 10.3348/kjr.2012.13.3.358. Epub 2012 Apr 17. Korean J Radiol. 2012. PMID: 22563276 Free PMC article. Review.
Cited by
-
Post-COVID-19 cholangiopathy: Systematic review.World J Methodol. 2023 Sep 20;13(4):296-322. doi: 10.5662/wjm.v13.i4.296. eCollection 2023 Sep 20. World J Methodol. 2023. PMID: 37771872 Free PMC article.
-
Imaging features of COVID-19-associated secondary sclerosing cholangitis on magnetic resonance cholangiopancreatography: a retrospective analysis.Insights Imaging. 2022 Aug 8;13(1):128. doi: 10.1186/s13244-022-01266-9. Insights Imaging. 2022. PMID: 35939241 Free PMC article.
References
-
- Scheppach W, Druge G, Wittenberg G, Mueller JG, Gassel AM, Gassel HJ, et al. Sclerosing cholangitis and liver cirrhosis after extrabiliary infections: report on three cases. Crit Care Med. 2001;29((2)):438–441. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
