

Using Single-Photon Emission Computerized Tomography on Patients With Positive Quantitative Electroencephalogram to Evaluate Chronic Mild Traumatic Brain Injury With Persistent Symptoms
- PMID: 35528740
- PMCID: PMC9074759
- DOI: 10.3389/fneur.2022.704844
Using Single-Photon Emission Computerized Tomography on Patients With Positive Quantitative Electroencephalogram to Evaluate Chronic Mild Traumatic Brain Injury With Persistent Symptoms
Abstract
Background: Following mild traumatic brain injury (mTBI), also known as concussion, many patients with chronic symptoms (>3 months post injury) receive conventional imaging such as computed tomography (CT) or magnetic resonance imaging (MRI). However, these modalities often do not show changes after mTBI. We studied the benefit of triaging patients with ongoing symptoms >3 months post injury by quantitative electroencephalography (qEEG) and then completing a brain single positron emission computed tomography (SPECT) to aid in diagnosis and early detection of brain changes.
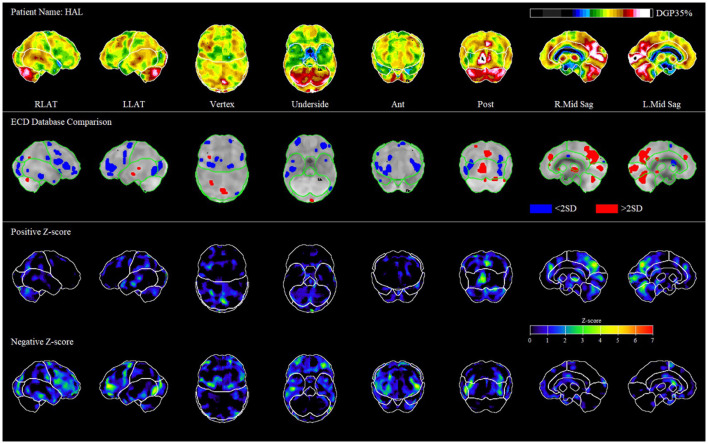
Methods: We conducted a retrospective case review of 30 outpatients with mTBI. The patients were assessed by a neurologist, consented, and received a qEEG, and if the qEEG was positive, they consented and received a brain SPECT scan. The cases and diagnostic tools were collectively reviewed by a multidisciplinary group of physicians in biweekly team meetings including neurology, nuclear medicine, psychiatry, neuropsychiatry, general practice psychotherapy, neuro-ophthalmology, and chiropractic providers. The team noted the cause of injury, post injury symptoms, relevant past medical history, physical examination findings, and diagnoses, and commented on patients' SPECT scans. We then analyzed the SPECT scans quantitatively using the 3D-SSP software.
Results: All the patients had cerebral perfusion abnormalities demonstrated by SPECT that were mostly undetectable by conventional imaging (CT/MRI). Perfusion changes were localized primarily in the cerebral cortex, basal ganglia, and cingulate cortex, and correlated with the patients' symptoms and examination findings. Qualitative and quantitative analyses yielded similar results. Most commonly, the patients experienced persistent headache, memory loss, concentration difficulties, depression, and cognitive impairment post mTBI. Because of their symptoms, most of the patients were unable to return to their previous employment and activity level.
Conclusion: Our findings outline the physical basis of neurological and psychiatric symptoms experienced by patients with mTBI. Increased detection of mTBI can lead to development of improved targeted treatments for mTBI and its various sequelae.
Keywords: concussion; neuropsychiatric symptoms; post-concussion syndrome (PCS); quantitative EEG (qEEG); single photon emission computed tomography (SPECT); traumatic brain injury (TBI).
Copyright © 2022 Gosset, Wagman, Pavel, Cohen, Tarzwell, Bruin, Siow, Numerow, Uszler, Rossiter-Thornton, McLean, Lierop, Waisman, Brown, Mansouri, Basile, Chaudhary and Mehdiratta.
Conflict of interest statement
MM has an interest in iScope Concussion and Pain Clinics, which uses qEEG and SPECT as part of the clinic. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Magnetic Resonance Imaging Application in the Area of Mild and Acute Traumatic Brain Injury: Implications for Diagnostic Markers?In: Kobeissy FH, editor. Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects. Boca Raton (FL): CRC Press/Taylor & Francis; 2015. Chapter 24. In: Kobeissy FH, editor. Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects. Boca Raton (FL): CRC Press/Taylor & Francis; 2015. Chapter 24. PMID: 26269902 Free Books & Documents. Review.
-
Microvascular and large vein abnormalities in young patients after mild head trauma and associated fatigue: A brain SPECT evaluation and posture dependence modeling.Clin Neurol Neurosurg. 2018 Jul;170:159-164. doi: 10.1016/j.clineuro.2018.05.019. Epub 2018 May 18. Clin Neurol Neurosurg. 2018. PMID: 29800829
-
Differences in cerebral perfusion deficits in mild traumatic brain injury and depression using single-photon emission computed tomography.Front Neurol. 2014 Aug 20;5:158. doi: 10.3389/fneur.2014.00158. eCollection 2014. Front Neurol. 2014. PMID: 25191305 Free PMC article.
-
[Mild traumatic brain injury and postconcussive syndrome: a re-emergent questioning].Encephale. 2012 Sep;38(4):329-35. doi: 10.1016/j.encep.2011.07.003. Epub 2011 Aug 31. Encephale. 2012. PMID: 22980474 Review. French.
-
Neuroimaging in Pediatric Patients with Mild Traumatic Brain Injury: Relating the Current 2018 Centers for Disease Control Guideline and the Potential of Advanced Neuroimaging Modalities for Research and Clinical Biomarker Development.J Neurotrauma. 2021 Jan 1;38(1):44-52. doi: 10.1089/neu.2020.7100. Epub 2020 Oct 21. J Neurotrauma. 2021. PMID: 32640874 Free PMC article. Review.
Cited by
-
Novel brain SPECT imaging unravels abnormal cerebral perfusion in patients with postural orthostatic tachycardia syndrome and cognitive dysfunction.Sci Rep. 2025 Jan 28;15(1):3487. doi: 10.1038/s41598-025-87748-4. Sci Rep. 2025. PMID: 39875497 Free PMC article.
-
Post-Traumatic Craniocervical Disorders From a Postural Control Perspective: A Narrative Review.Brain Neurorehabil. 2023 Jul 7;16(2):e15. doi: 10.12786/bn.2023.16.e15. eCollection 2023 Jul. Brain Neurorehabil. 2023. PMID: 37554255 Free PMC article. Review.
-
Traumatic brain injuries: a neuropsychological review.Front Behav Neurosci. 2024 Oct 8;18:1326115. doi: 10.3389/fnbeh.2024.1326115. eCollection 2024. Front Behav Neurosci. 2024. PMID: 39444788 Free PMC article. Review.
-
Brain Punch: K-1 Fights Affect Brain Wave Activity in Professional Kickboxers.Sports Med. 2024 Dec;54(12):3169-3179. doi: 10.1007/s40279-024-02082-5. Epub 2024 Aug 7. Sports Med. 2024. PMID: 39112919 Free PMC article.
References
-
- Kay T, Harrington DE, Adams R, Anderson T, Berrol S, Cicerone K, et al. . Definition of mild traumatic brain injury. J Head Trauma Rehabil. (1993) 8:86–7. 10.1097/00001199-199309000-00010 - DOI
-
- Rathbone M, Mehdiratta M, Finlayson H. Mild head injury. Can J Cardiol. (2000) 15:76–93
LinkOut - more resources
Full Text Sources
Miscellaneous