

Trends of Clinical Outcomes of Patients with Advanced Hepatocellular Carcinoma Treated with First-Line Sorafenib in Randomized Controlled Trials
- PMID: 35528745
- PMCID: PMC9021659
- DOI: 10.1159/000521625
Trends of Clinical Outcomes of Patients with Advanced Hepatocellular Carcinoma Treated with First-Line Sorafenib in Randomized Controlled Trials
Abstract
Background: Sorafenib has consistently served as the control arm in multiple randomized clinical trials (RCTs) evaluating novel therapies for advanced hepatocellular carcinoma (HCC) for more than a decade. Analyzing trends in clinical outcomes of patients treated with sorafenib for the same indication over time offers the opportunity for unique insight into the evolution of clinical trial conduct and potential non-drug factors impacting outcomes.
Methods: We identified RCTs in patients with treatment-naïve advanced HCC where sorafenib was compared to another systemic therapy or placebo. We extracted trial-level demographic, clinicopathologic, and outcome data (overall survival [OS], progression-free survival [PFS], objective response rate [ORR], and duration of therapy). Sample-weighted linear regression was used to identify temporal trends with significance set at p ≤ 0.05.
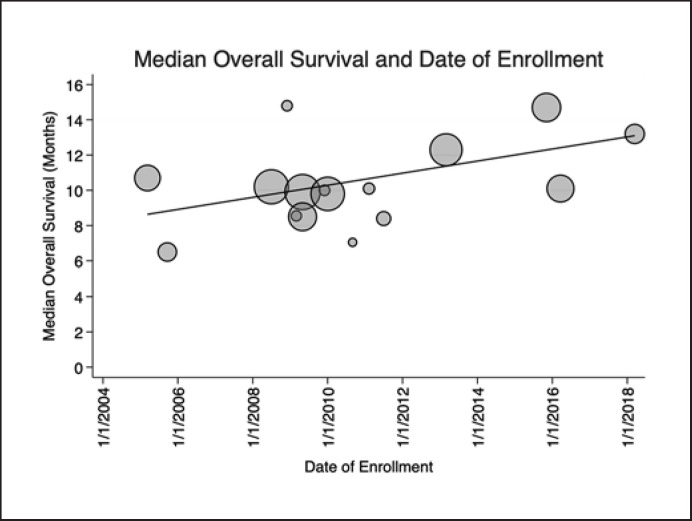
Results: Sixteen RCTs (9 phase III and 7 phase II) enrolling 4,086 patients treated with sorafenib were included in the analysis. Included trials enrolled patients from 2005 to 2019. OS has significantly improved by 4.5 months from 2005 to 2019 (p = 0.048) over time. Thirteen studies provided data on PFS using Response Evaluation Criteria in Solid Tumors (RECIST) 1.1, with no significant change over time (p = 0.69). ORR assessed by RECIST 1.1 has significantly improved by 6.0% over time (p = 0.003). Median duration of therapy with sorafenib has decreased by 53% since the enrollment of the first clinical trial in 2005, from 23.1 weeks to 12.2 weeks (p = 0.0037). There was no significant change in patient demographics were identified over time to explain the OS findings.
Conclusion: The median OS of patients with advanced HCC treated with sorafenib has improved significantly over 15 years. At the same time, the median duration of therapy with sorafenib has decreased. The reason for these findings was not explained by changing demographics of patients enrolled in these trials and has implications for ongoing clinical trials.
Keywords: Cancer outcomes; Clinical trials; Hepatocellular carcinoma; Sorafenib.
Copyright © 2021 by S. Karger AG, Basel.
Conflict of interest statement
M.Y. reports receiving research grants from Incyte, Bristol Myers Squibb, and Exelixis and is a consultant for AstraZeneca, Eisai, Exelixis, and Genentech. The other authors declare no competing interests.
Figures



Similar articles
-
Survival Trends in Sorafenib for Advanced Hepatocellular Carcinoma: A Reconstructed Individual Patient Data Meta-Analysis of Randomized Trials.Liver Cancer. 2023 Mar 28;12(5):445-456. doi: 10.1159/000529824. eCollection 2023 Oct. Liver Cancer. 2023. PMID: 37901764 Free PMC article.
-
Comparative Efficacy of Cabozantinib and Regorafenib for Advanced Hepatocellular Carcinoma.Adv Ther. 2020 Jun;37(6):2678-2695. doi: 10.1007/s12325-020-01378-y. Epub 2020 May 18. Adv Ther. 2020. PMID: 32424805 Free PMC article.
-
Early Changes in DCE-MRI Biomarkers May Predict Survival Outcomes in Patients with Advanced Hepatocellular Carcinoma after Sorafenib Failure: Two Prospective Phase II Trials.Cancers (Basel). 2021 Oct 1;13(19):4962. doi: 10.3390/cancers13194962. Cancers (Basel). 2021. PMID: 34638446 Free PMC article.
-
Early predictive value of circulating biomarkers for sorafenib in advanced hepatocellular carcinoma.Expert Rev Mol Diagn. 2022 Mar;22(3):361-378. doi: 10.1080/14737159.2022.2049248. Epub 2022 Mar 11. Expert Rev Mol Diagn. 2022. PMID: 35234564 Review.
-
Outcomes of hepatocellular carcinoma patients treated with sorafenib: a meta-analysis of Phase III trials.Future Oncol. 2019 Oct;15(29):3411-3422. doi: 10.2217/fon-2019-0287. Epub 2019 Oct 7. Future Oncol. 2019. PMID: 31588789
Cited by
-
Survival Trends in Sorafenib for Advanced Hepatocellular Carcinoma: A Reconstructed Individual Patient Data Meta-Analysis of Randomized Trials.Liver Cancer. 2023 Mar 28;12(5):445-456. doi: 10.1159/000529824. eCollection 2023 Oct. Liver Cancer. 2023. PMID: 37901764 Free PMC article.
-
Clinical Characteristics, Prognostic Factors and Therapeutic Strategies in Gastric Cancer Patients With Bone Metastasis: A Retrospective Analysis.Cancer Med. 2025 Mar;14(6):e70781. doi: 10.1002/cam4.70781. Cancer Med. 2025. PMID: 40105370 Free PMC article.
-
New Opportunities in the Systemic Treatment of Hepatocellular Carcinoma-Today and Tomorrow.Int J Mol Sci. 2024 Jan 25;25(3):1456. doi: 10.3390/ijms25031456. Int J Mol Sci. 2024. PMID: 38338736 Free PMC article. Review.
-
Adjuvant Sorafenib for Postoperative Patients with Hepatocellular Carcinoma and Macrovascular Invasion.Curr Oncol. 2023 Nov 28;30(12):10134-10141. doi: 10.3390/curroncol30120737. Curr Oncol. 2023. PMID: 38132371 Free PMC article.
-
Duration of treatment in oncology clinical trials: does the duration change when the same drug moves from the experimental arm to the control arm?ESMO Open. 2022 Jun;7(3):100480. doi: 10.1016/j.esmoop.2022.100480. Epub 2022 Apr 22. ESMO Open. 2022. PMID: 35468562 Free PMC article.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68((6)):394–424. - PubMed
-
- Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc J-F, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359((4)):378–390. - PubMed
-
- Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10((1)):25–34. - PubMed
-
- Keating GM. Sorafenib: a review in hepatocellular carcinoma. Target Oncol. 2017;12((2)):243–253. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
