

Copeptin Levels Before and After Transsphenoidal Surgery for Cushing Disease: A Potential Early Marker of Remission
- PMID: 35528828
- PMCID: PMC9070476
- DOI: 10.1210/jendso/bvac053
Copeptin Levels Before and After Transsphenoidal Surgery for Cushing Disease: A Potential Early Marker of Remission
Abstract
Context: Arginine-vasopressin and CRH act synergistically to stimulate secretion of ACTH. There is evidence that glucocorticoids act via negative feedback to suppress arginine-vasopressin secretion.
Objective: Our hypothesis was that a postoperative increase in plasma copeptin may serve as a marker of remission of Cushing disease (CD).
Design: Plasma copeptin was obtained in patients with CD before and daily on postoperative days 1 through 8 after transsphenoidal surgery. Peak postoperative copeptin levels and Δcopeptin values were compared among those in remission vs no remission.
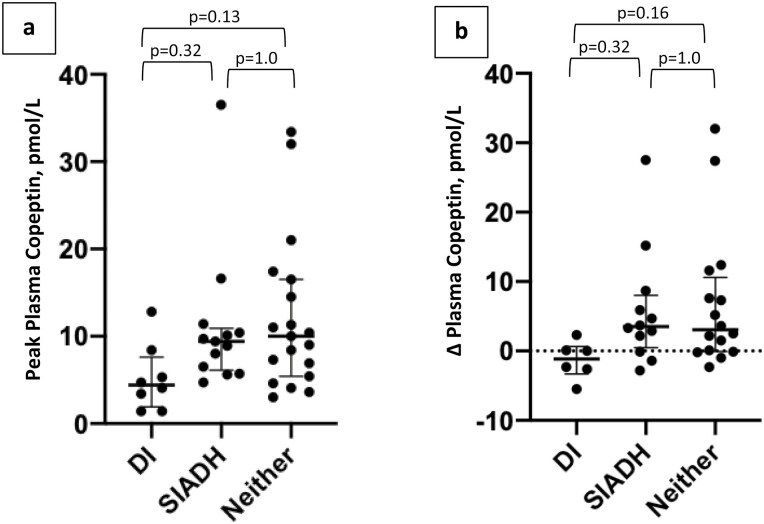
Results: Forty-four patients (64% female, aged 7-55 years) were included, and 19 developed neither diabetes insipidus (DI) or syndrome of inappropriate anti-diuresis (SIADH). Thirty-three had follow-up at least 3 months postoperatively. There was no difference in peak postoperative copeptin in remission (6.1 pmol/L [4.3-12.1]) vs no remission (7.3 pmol/L [5.4-8.4], P = 0.88). Excluding those who developed DI or SIADH, there was no difference in peak postoperative copeptin in remission (10.2 pmol/L [6.9-21.0]) vs no remission (5.4 pmol/L [4.6-7.3], P = 0.20). However, a higher peak postoperative copeptin level was found in those in remission (14.6 pmol/L [±10.9] vs 5.8 (±1.4), P = 0.03]) with parametric testing. There was no difference in the Δcopeptin by remission status.
Conclusions: A difference in peak postoperative plasma copeptin as an early marker to predict remission of CD was not consistently present, although the data point to the need for a larger sample size to further evaluate this. However, the utility of this test may be limited to those who develop neither DI nor SIADH postoperatively.
Keywords: Cushing disease; copeptin; cortisol; remission.
Published by Oxford University Press on behalf of the Endocrine Society 2022.
Figures






References
-
- Kaiser U, Ho KKY. Chapter 8: pituitary physiology and diagnostic evaluation. In: Melmed S, Larsen PR, Kronenberg H, eds. Williams Textbook of Endocrinology, P.K. Elsevier: Philadelphia; 2016:176–231.
-
- Katan M, Christ-Crain M. The stress hormone copeptin: a new prognostic biomarker in acute illness. Swiss Med Wkly. 2010;140:w13101. - PubMed
LinkOut - more resources
Full Text Sources