

Case Reports
doi: 10.3941/jrcr.v16i3.4191.
eCollection 2022 Mar.
Sarcoidosis with hepatic involvement in a 60-year-old patient
Affiliations
- PMID: 35529425
- PMCID: PMC9063835
- DOI: 10.3941/jrcr.v16i3.4191
Item in Clipboard
Case Reports
Sarcoidosis with hepatic involvement in a 60-year-old patient
J Radiol Case Rep.
.
Abstract
Hepatic involvement of sarcoidosis is usually hard to detect on radiological imaging. We present a case of a 60-year-old female with symptoms of pulmonary sarcoidosis. Subsequent imaging work-up showed diffuse hepatic granulomas consistent with abdominal involvement of sarcoidosis. A literature review regarding hepatic sarcoidosis is provided and radiological appearances as well as considerations for differential diagnosis are described.
Keywords: Abdominal sarcoidosis; Computed tomography; Hepatic granulomas; Hepatic sarcoidosis; Sarcoidosis.
Copyright Journal of Radiology Case Reports.
Figures
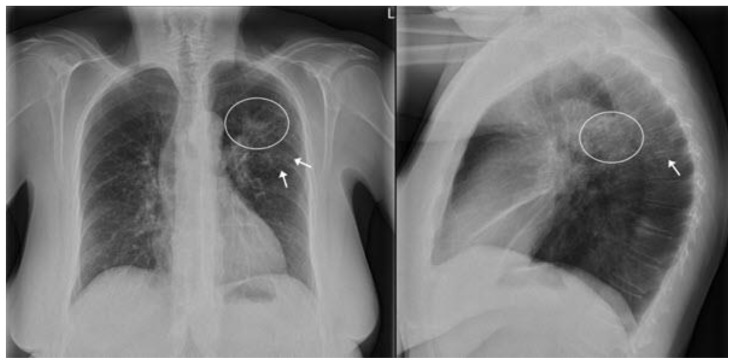
60-year-old female with pulmonary abnormalities due to sarcoidosis. TECHNIQUE: X-thorax, PA and lateral view. (General Electric (GE), PA: 125 kV, 2.6 mAs. Lateral: 125 kV, 4.5 mAs). FINDINGS: There is a small left perihilar consolidation (circles) along with multiple fine reticulations in both upper lobes (arrow).
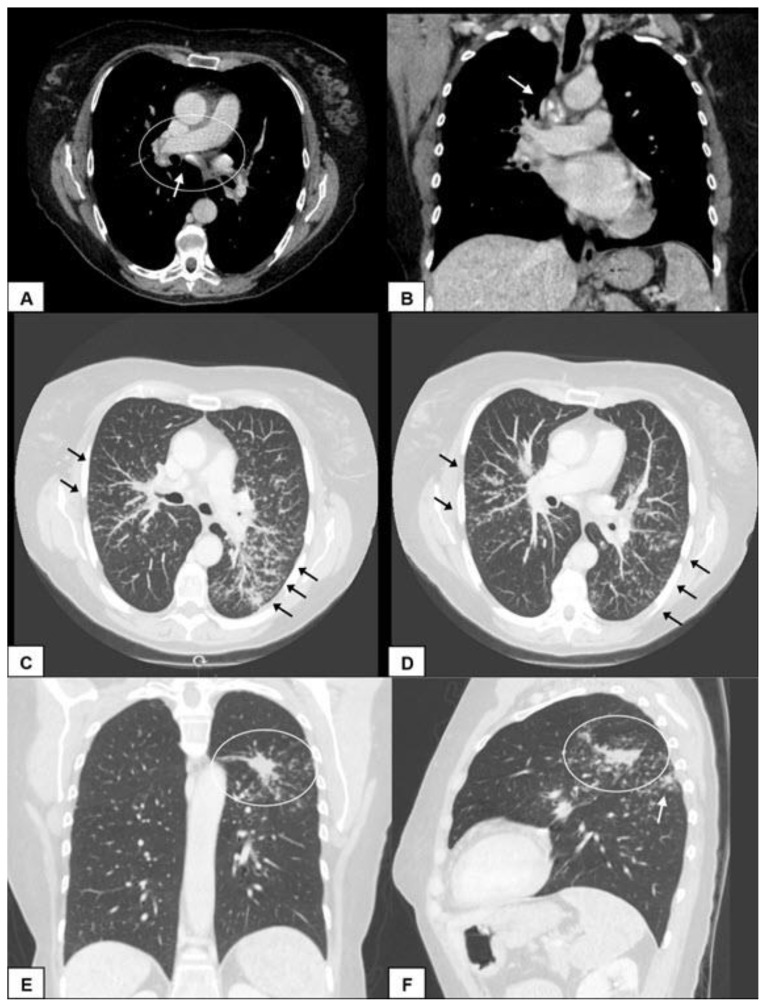
60-year-old female with lymphatic and pulmonary abnormalities due to sarcoidosis. TECHNIQUE: Contrast enhanced computed tomography (CECT) scan of the thorax/abdomen (only thorax shown in this figure). (General Electric (GE), 120 kV, CTDIvol: 3.44 mGy, DLP: 152 mGy*cm. 1 mm slice thickness, 90 cc visipaque 320). FINDINGS: A and B) Axial and coronal images of the mediastinum showing bilateral hilar and mediastinal lymphadenopathy (circle). Some of the lymph nodes were partially calcified (arrows). C and D) Axial images in maximum intensity projection (MIP) setting showing multiple fine nodules along the subpleural surfaces and fissures and along the interlobular septa and peribronchovascular bundles (arrows), consistent with a perilymphatic distribution pattern. E and F) Coronal and sagittal images showing a consolidation in the posterior aspect of the left upper lobe and some smaller consolidations in the apical left lower lobe (arrow).
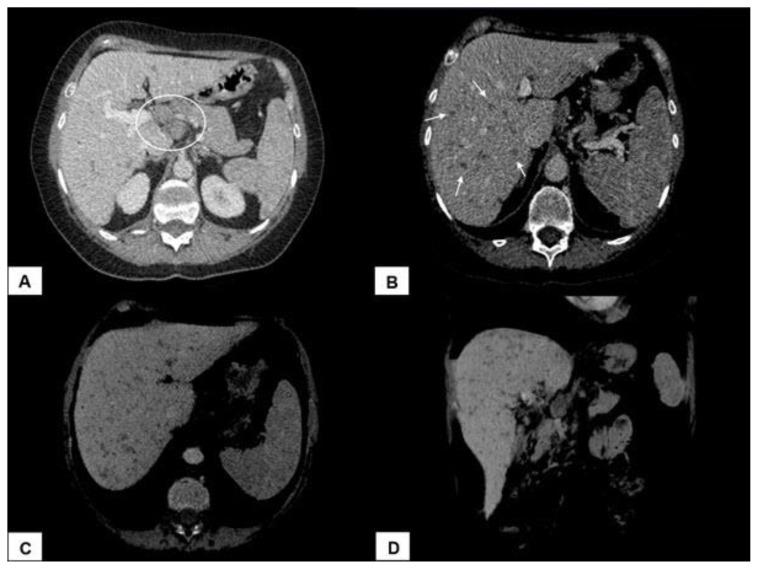
60-year-old female with hepatic and splenic granulomas and perihepatic lymphadenopathy due to abdominal involvement of sarcoidosis. TECHNIQUE: Contrast enhanced computed tomography (CECT) scan of the thorax/abdomen (only upper abdomen shown in this figure). (General Electric (GE), 120 kV, CTDIvol: 3.44 mGy, DLP: 152 mGy*cm. 1 mm slice thickness, 90 cc visipaque 320). FINDINGS: A) Axial image showing extensive lymphadenopathy in the porta hepatis (circle). B) Axial image showing significant enlargement of the liver. The liver parenchyma is characterized by diffuse inhomogeneous enhancement caused by multiple hardly distinctive and partially confluent hypoattenuating nodules, ranging in size from 1–10 mm (arrows). C and D) The dispersed distribution of hepatic nodules is better seen in minimum intensity projection (Min-IP) setting. The same pattern of fine nodules could be identified in the slightly enlarged spleen.
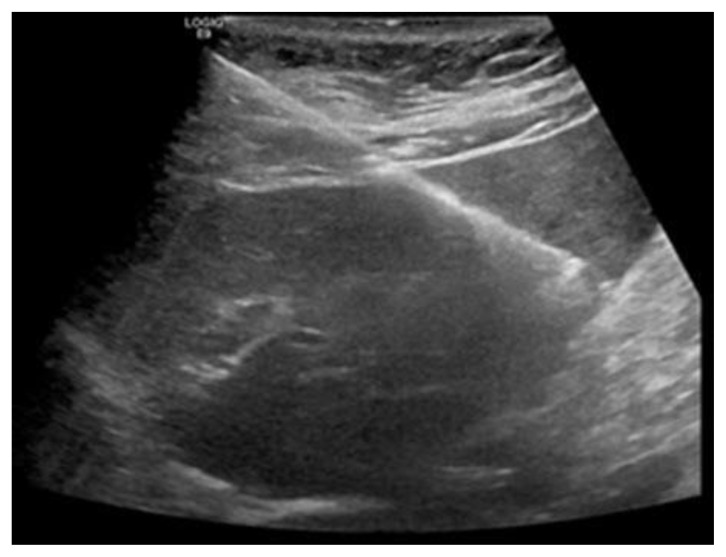
60-year-old female with hepatic involvement of sarcoidosis. TECHNIQUE: Standard ultrasound procedure (General Electric (GE)), with ultrasound guided biopsy of the liver. FINDINGS: There is subtle coarsening of the liver parenchymal appearance without discrete nodules. Biopsy was performed in liver segment II/ III.
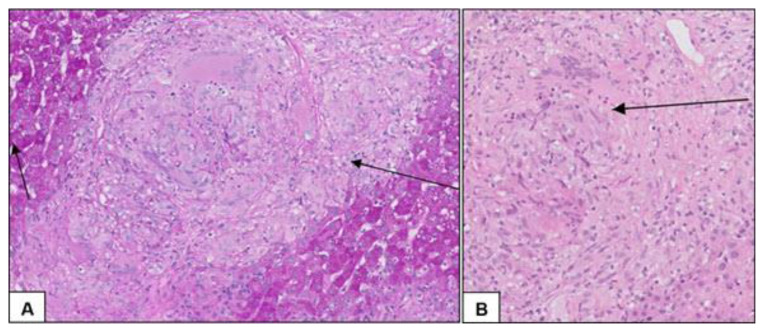
Liver biopsy specimen of a 60-year-old female with hepatic involvement of sarcoidosis. TECHNIQUE: Microscopic image after Periodic acid-Schiff (PAS) staining. FINDINGS: A) Aggregates of epithelioid histiocytes with regular margins forming multiple non-caseating granulomas within the portal tract as well as in the periportal areas of the liver. Short arrow: normal liver tissue. Long arrow: granuloma. B) Close view of a granuloma: aggregates of epithelioid cells, which fuse together to form multinucleated giant cells (long arrow).
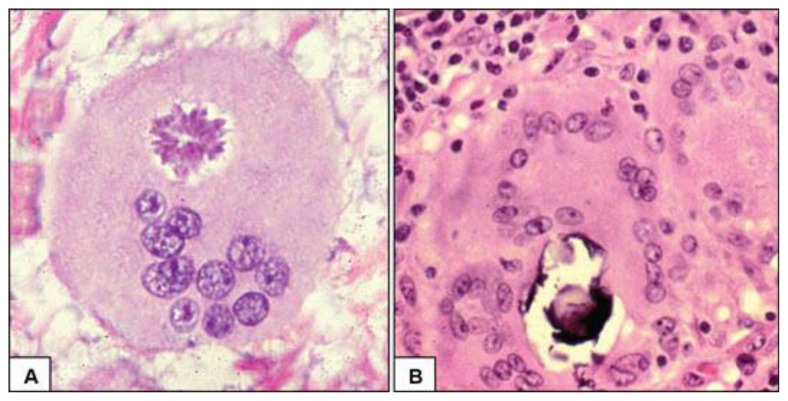
Histopathological findings in sarcoidosis. A) Sarcoid granuloma with an asteroid body. B) Well-formed sarcoid granuloma with multinucleated giant cells and a Schaumann body. Source: Laga AC, Allen TC, Bedrossian C, et al. Noncellular structures. In: Color Atlas and Text of Pulmonary Pathology, 2nd Edition, Cagle PT, Allen TC, Barrios R, et al (Eds), Philadelphia: Lippincott Williams & Wilkins, 2008.
References
-
- Judson MA.Extrapulmonary sarcoidosis Semin Respir Crit Care Med 2007. Feb28183–101. - PubMed
-
- Baughman RP, Teirstein AS, Judson MA, et al. Case Control Etiologic Study of Sarcoidosis (ACCESS) research group. Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med. 2001 Nov 15;164(10 Pt 1):1885–9. - PubMed
-
- Rybicki BA, Major M, Popovich J, Jr, Maliarik MJ, Iannuzzi MC. Racial differences in sarcoidosis incidence: a 5-year study in a health maintenance organization. Am J Epidemiol. 1997 Feb 1;145(3):234–41. - PubMed
-
- Culver DA. Sarcoidosis. Immunol Allergy Clin North Am. 2012 Nov;32(4):487–511. - PubMed
-
- Kahi CJ, Saxena R, Temkit M, Canlas K, Roberts S, Knox K, Wilkes D, Kwo PY. Hepatobiliary disease in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2006 Jun;23(2):117–23. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical