

Optimal Intervention for Initial Treatment of Anastomotic Biliary Complications After Right Lobe Living Donor Liver Transplantation
- PMID: 35529595
- PMCID: PMC9073559
- DOI: 10.3389/ti.2022.10044
Optimal Intervention for Initial Treatment of Anastomotic Biliary Complications After Right Lobe Living Donor Liver Transplantation
Abstract
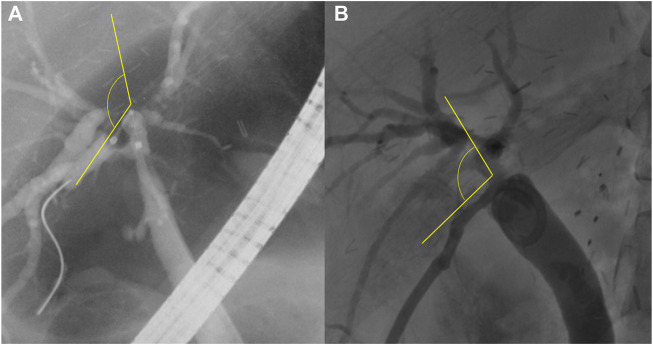
Background: This study evaluated endoscopic retrograde cholangiopancreatography (ERCP) and percutaneous transhepatic biliary drainage (PTBD) as interventions for patients with anastomotic biliary complications (ABC) after living donor liver transplantation (LDLT). Methods: Prospectively collected data of patients who were diagnosed with ABC after LDLT between January 2013 and June 2017 were retrospectively reviewed. Results: There were 57 patients who underwent LDLT with a right liver graft using duct-to-duct biliary reconstruction and experienced ABC. Among the patients with RAD involvement, there were no significant differences in the intervention success (p = 0.271) and patency rates (p = 0.267) between ERCP and PTBD. Similarly, among the patients with RPD involvement, there were no significant differences in the intervention success (p = 0.148) and patency rates (p = 0.754) between the two procedures. Graft bile duct variation (p = 0.013) and a large angle between the recipient and graft bile duct (R-G angle) (p = 0.012) significantly increased the likelihood of failure of ERCP in the RAD. When the R-G angle was greater than 47.5°, the likelihood of ERCP failure increased. Conclusion: We recommend PTBD when graft bile duct variation is presented in patients with RAD involvement and/or when the R-G angle is greater than 47.5°.
Keywords: anastomotic biliary complications; endoscopic retrograde cholangiography; living donor liver transplantation; percutaneous transhepatic biliary drainage; right anterior hepatic duct; right posterior hepatic duct.
Copyright © 2022 Kim, Hong, Woo, Cho, Lee, Yoon, Choi, Yi, Lee and Suh.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Optimal Biliary Drainage for Patients With Biliary Anastomotic Strictures After Right Lobe Living Donor Liver Transplantation.Liver Transpl. 2019 Aug;25(8):1209-1219. doi: 10.1002/lt.25472. Epub 2019 Jul 4. Liver Transpl. 2019. PMID: 30980451
-
Percutaneous transhepatic biliary drainage may serve as a successful rescue procedure in failed cases of endoscopic therapy for a post-living donor liver transplantation biliary stricture.Gastrointest Endosc. 2009 Jan;69(1):38-46. doi: 10.1016/j.gie.2008.03.1113. Epub 2008 Jul 16. Gastrointest Endosc. 2009. PMID: 18635177
-
Percutaneous Transhepatic Biliary Drainage for Biliary Stricture After Endotherapy Failure in Living Donor Liver Transplantation: A Single-Centre Experience from India.J Clin Exp Hepatol. 2019 Nov-Dec;9(6):684-689. doi: 10.1016/j.jceh.2019.03.004. Epub 2019 Mar 25. J Clin Exp Hepatol. 2019. PMID: 31889748 Free PMC article.
-
Prevention and management of biliary anastomotic stricture in right-lobe living-donor liver transplantation.J Gastroenterol Hepatol. 2014 Oct;29(10):1756-63. doi: 10.1111/jgh.12648. J Gastroenterol Hepatol. 2014. PMID: 24909190 Review.
-
Bile duct kinking after adult living donor liver transplantation: Case reports and literature review.J Dig Dis. 2015 Oct;16(10):610-5. doi: 10.1111/1751-2980.12263. J Dig Dis. 2015. PMID: 26031803 Review.
Cited by
-
Feasibility and safety of a novel 3D-printed biodegradable biliary stent in an in vivo porcine model: a preliminary study.Sci Rep. 2022 Sep 23;12(1):15875. doi: 10.1038/s41598-022-19317-y. Sci Rep. 2022. PMID: 36151222 Free PMC article.
-
Management of biliary complications after LDLT.Updates Surg. 2024 Sep 14. doi: 10.1007/s13304-024-01988-z. Online ahead of print. Updates Surg. 2024. PMID: 39276196
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical