

Chronic Inflammatory Placental Disorders Associated With Recurrent Adverse Pregnancy Outcome
- PMID: 35529853
- PMCID: PMC9072631
- DOI: 10.3389/fimmu.2022.825075
Chronic Inflammatory Placental Disorders Associated With Recurrent Adverse Pregnancy Outcome
Abstract
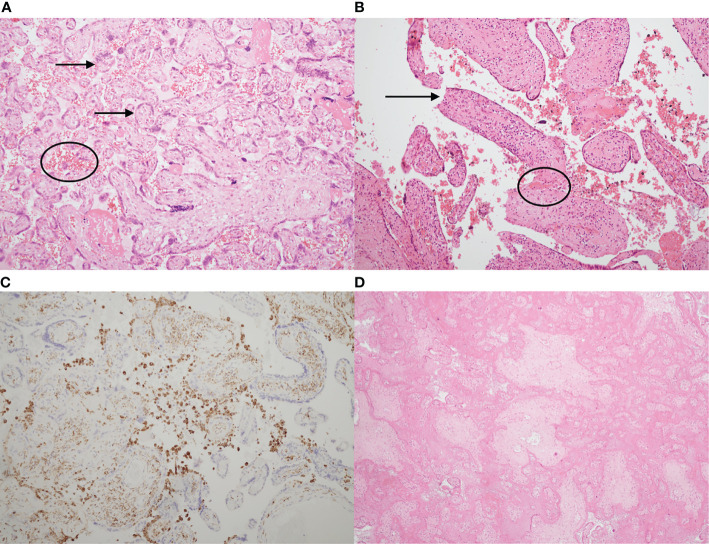
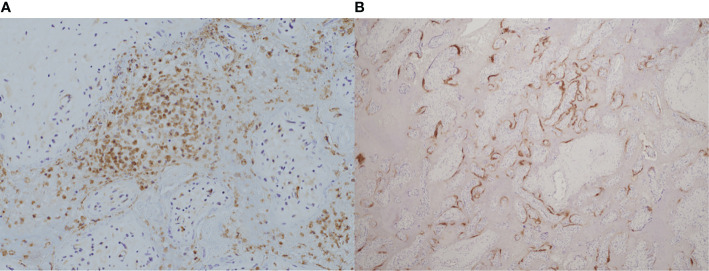
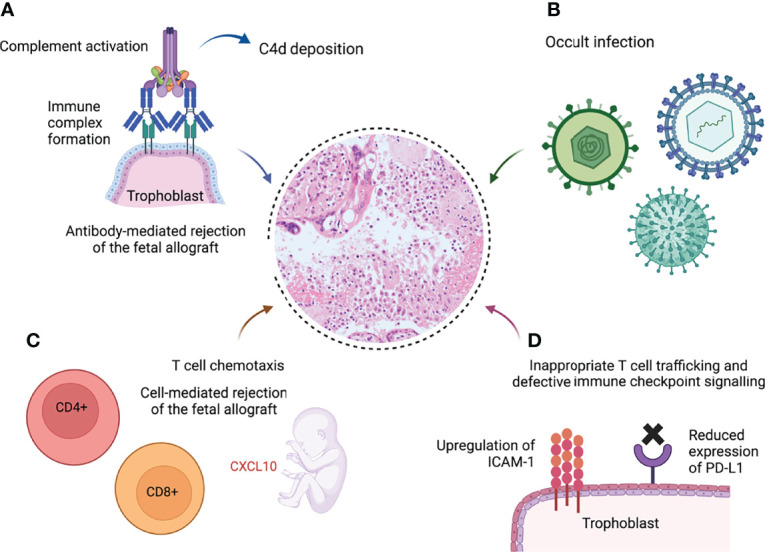
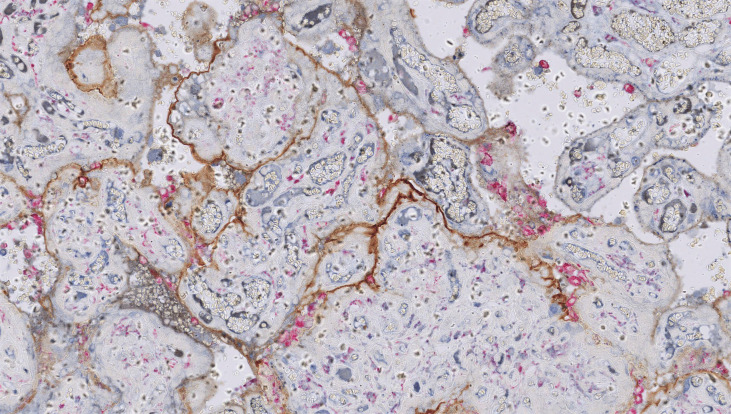
Chronic inflammatory placental disorders are a group of rare but devastating gestational syndromes associated with adverse pregnancy outcome. This review focuses on three related conditions: villitis of unknown etiology (VUE), chronic histiocytic intervillositis (CHI) and massive perivillous fibrin deposition (MPFD). The hallmark of these disorders is infiltration of the placental architecture by maternal immune cells and disruption of the intervillous space, where gas exchange between the mother and fetus occurs. Currently, they can only be detected through histopathological examination of the placenta after a pregnancy has ended. All three are associated with a significant risk of recurrence in subsequent pregnancies. Villitis of unknown etiology is characterised by a destructive infiltrate of maternal CD8+ T lymphocytes invading into the chorionic villi, combined with activation of fetal villous macrophages. The diagnosis can only be made when an infectious aetiology has been excluded. VUE becomes more common as pregnancy progresses and is frequently seen with normal pregnancy outcome. However, severe early-onset villitis is usually associated with fetal growth restriction and recurrent pregnancy loss. Chronic histiocytic intervillositis is characterised by excessive accumulation of maternal CD68+ histiocytes in the intervillous space. It is associated with a wide spectrum of adverse pregnancy outcomes including high rates of first-trimester miscarriage, severe fetal growth restriction and late intrauterine fetal death. Intervillous histiocytes can also accumulate due to infection, including SARS-CoV-2, although this infection-induced intervillositis does not appear to recur. As with VUE, the diagnosis of CHI requires exclusion of an infectious cause. Women with recurrent CHI and their families are predisposed to autoimmune diseases, suggesting CHI may have an alloimmune pathology. This observation has driven attempts to prevent CHI with a wide range of maternal immunosuppression. Massive perivillous fibrin deposition is diagnosed when >25% of the intervillous space is occupied by fibrin, and is associated with fetal growth restriction and late intrauterine fetal death. Although not an inflammatory disorder per se, MPFD is frequently seen in association with both VUE and CHI. This review summarises current understanding of the prevalence, diagnostic features, clinical consequences, immune pathology and potential prophylaxis against recurrence in these three chronic inflammatory placental syndromes.
Keywords: CD8+ T lymphocytes; allograft rejection; chronic histiocytic intervillositis; chronic placental inflammation; fetal growth restriction; massive perivillous fibrin deposition; stillbirth; villitis of unknown etiology.
Copyright © 2022 Cornish, McDonnell and Williams.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- NHS England . Saving Babies’ Lives Version Two: A Care Bundle for Reducing Perinatal Mortality (2019). Available at: https://www.england.nhs.uk/wp-content/uploads/2019/03/Saving-Babies-Live....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous