

Hyperfractionated-Accelerated Reirradiation with Proton Therapy for Radiation-Associated Breast Angiosarcoma
- PMID: 35530187
- PMCID: PMC9009453
- DOI: 10.14338/IJPT-21-00031.1
Hyperfractionated-Accelerated Reirradiation with Proton Therapy for Radiation-Associated Breast Angiosarcoma
Abstract
Purpose: Radiation-associated angiosarcoma (RAAS) is a rare complication among patients treated with radiation therapy for breast cancer. Hyperfractionated-accelerated reirradiation (HART) improves local control after surgery. Proton therapy may further improve the therapeutic ratio by mitigating potential toxicity.
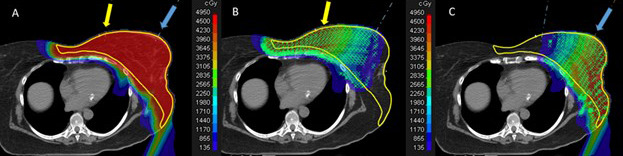
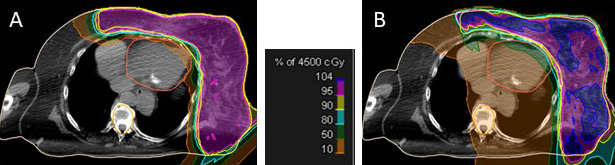
Materials and methods: Six patients enrolled in a prospective registry with localized RAAS received HART with proton therapy between 2015 and 2021. HART was delivered twice or thrice daily in fraction sizes of 1.5 or 1.0 Gy, respectively. All patients received 45 Gy to a large elective volume followed by boosts to a median dose of 65 (range, 60-75) Gy. Toxicity was recorded prospectively by using the Common Terminology Criteria for Adverse Events, version 4.0.
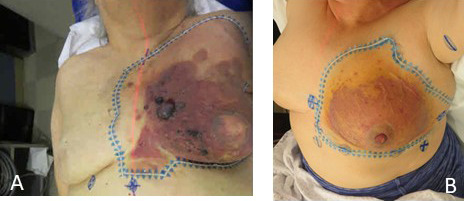
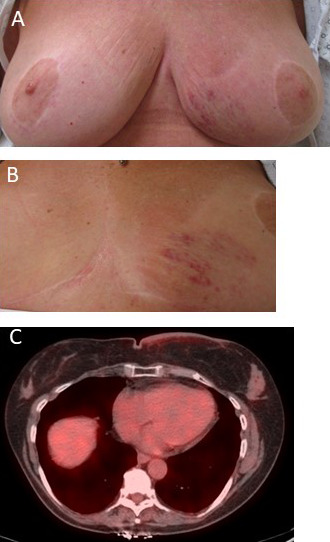
Results: The median follow-up duration was 1.5 (range, 0.25-2.9) years. The median age at RAAS diagnosis was 73 (range, 60-83) years with a median latency of 8.9 (range, 5-14) years between radiation therapy completion and RAAS diagnosis. The median mean heart dose was 2.2 (range, 0.1-4.96) Gy. HART was delivered postoperatively (n = 1), preoperatively (n = 3), preoperatively for local recurrence after initial management with mastectomy (n = 1), and as definitive treatment (n = 1). All patients had local control of disease throughout follow-up. Three of 4 patients treated preoperatively had a pathologic complete response. The patient treated definitively had a complete metabolic response on her posttreatment PET/CT (positron emission tomography-computed tomography) scan. Two patients developed distant metastatic disease despite local control and died of their disease. Acute grade 3 toxicity occurred in 3 patients: 2 patients undergoing preoperative HART experienced wound dehiscence and 1 postoperatively developed grade 3 wound infection, which resolved.
Conclusion: HART with proton therapy appears effective for local control of RAAS with a high rate of pathologic complete response and no local recurrences to date. However, vigilant surveillance for distant metastasis should occur. Toxicity is comparable to that in photon/electron series. Proton therapy for RAAS may maximize normal tissue sparing in this large-volume reirradiation setting.
Keywords: angiosarcoma; breast cancer; cancer outcomes; hyperfractionated radiation; second malignancies.
©Copyright 2021 The Author(s).
Conflict of interest statement
Conflicts of Interest: Nancy P. Mendenhall, MD, is Editor-in-Chief of the International Journal of Particle Therapy. The authors have no additional conflicts of interest to disclose.
Figures

Similar articles
-
Radical chest wall resection and hyperfractionated accelerated radiotherapy for radiation-associated angiosarcoma of the breast: A safe and effective treatment strategy.Breast J. 2018 May;24(3):245-252. doi: 10.1111/tbj.12886. Epub 2017 Aug 27. Breast J. 2018. PMID: 28845531
-
Preoperative hyperfractionated chemoradiation for locally recurrent rectal cancer in patients previously irradiated to the pelvis: A multicentric phase II study.Int J Radiat Oncol Biol Phys. 2006 Mar 15;64(4):1129-39. doi: 10.1016/j.ijrobp.2005.09.017. Epub 2006 Jan 18. Int J Radiat Oncol Biol Phys. 2006. PMID: 16414206 Clinical Trial.
-
Hyperfractionated accelerated radiation therapy for non-small cell lung cancer: clinical phase I/II trial.Int J Radiat Oncol Biol Phys. 1997 Oct 1;39(3):545-52. doi: 10.1016/s0360-3016(97)00332-5. Int J Radiat Oncol Biol Phys. 1997. PMID: 9336130 Clinical Trial.
-
How successful is high-dose (> or = 60 Gy) reirradiation using mainly external beams in salvaging local failures of nasopharyngeal carcinoma?Int J Radiat Oncol Biol Phys. 1998 Mar 1;40(4):897-913. doi: 10.1016/s0360-3016(97)00854-7. Int J Radiat Oncol Biol Phys. 1998. PMID: 9531376 Review.
-
[Hyperfractionated reirradiation after salvage surgery in cervico-facial carcinoma. Result of a pilot study in 14 patients].Cancer Radiother. 1997;1(1):68-73. doi: 10.1016/s1278-3218(97)84058-9. Cancer Radiother. 1997. PMID: 9265536 Review. French.
Cited by
-
Comparative Evaluation of Proton Therapy and Volumetric Modulated Arc Therapy for Brachial Plexus Sparing in the Comprehensive Reirradiation of High-Risk Recurrent Breast Cancer.Adv Radiat Oncol. 2023 Aug 18;9(2):101355. doi: 10.1016/j.adro.2023.101355. eCollection 2024 Feb. Adv Radiat Oncol. 2023. PMID: 38405315 Free PMC article.
-
Radiation-Associated Angiosarcoma of the Breast: The State of the Art of a Rare and Aggressive Disease.J Pers Med. 2024 Aug 14;14(8):859. doi: 10.3390/jpm14080859. J Pers Med. 2024. PMID: 39202050 Free PMC article. Review.
References
-
- Smith TL, Morris CG, Mendenhall NP. Angiosarcoma after breast-conserving therapy: long-term disease control and late effects with hyperfractionated accelerated re-irradiation (HART) Acta Oncol . 2014;53:235–41. - PubMed
-
- Palta M, Morris CG, Grobmyer SR, Copeland EM, III, Mendenhall NP. Angiosarcoma after breast-conserving therapy: long-term outcomes with hyperfractionated radiotherapy. Cancer . 2010;116:1872–8. - PubMed
-
- Hui A, Henderson M, Speakman D, Skandarajah A. Angiosarcoma of the breast: a difficult surgical challenge. Breast . 2012;21:584–9. - PubMed
LinkOut - more resources
Full Text Sources