

COVID-Induced Fulminant Myocarditis
- PMID: 35530896
- PMCID: PMC9076055
- DOI: 10.7759/cureus.23894
COVID-Induced Fulminant Myocarditis
Abstract
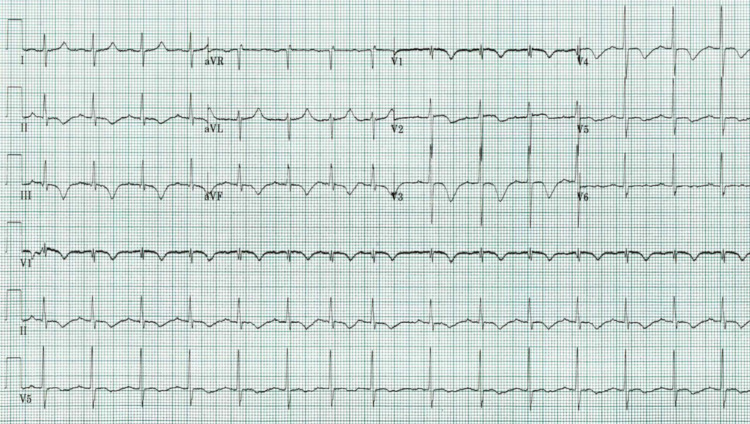
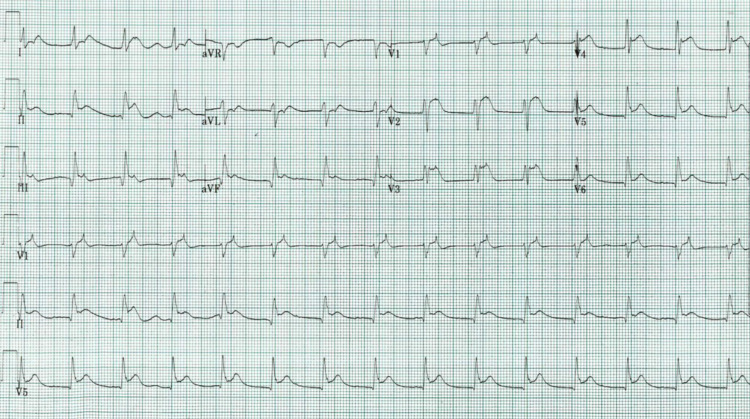
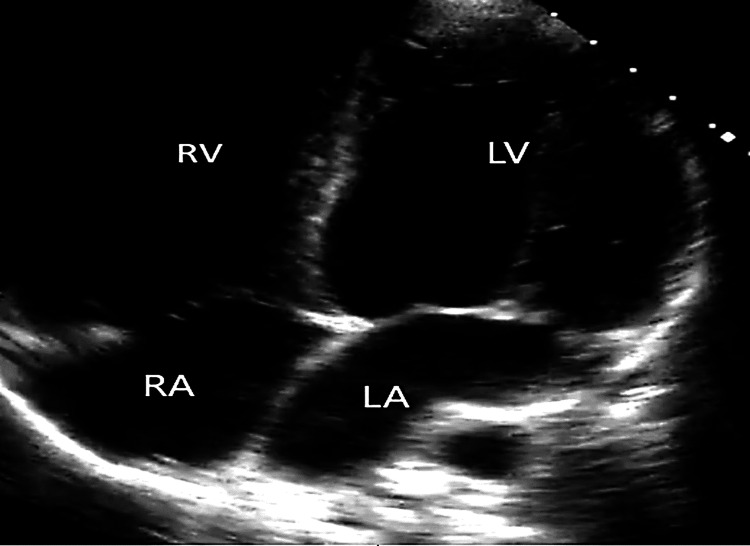
Viral-induced myocarditis has different presentations, from being asymptomatic to fatal arrhythmias. It is crucial to recognize and treat this condition early to improve morbidity and mortality. We report a case of a 56-year-old male who tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) three days ago and presented with syncope. The physical exam was relevant for right eyebrow laceration, tachycardia, and hypotension that responded to intravenous fluid, but two hours later, he had mental status changes, bradycardia, hypotension, and cardiac arrest. His repeated electrocardiogram (ECG) showed diffuse ST-segment elevation. Troponemia was evident in his blood work. Point-of-care ultrasound (POCUS) at the bedside showed dilated cardiomyopathy. Unfortunately, the patient re-arrested and needed advanced cardiovascular life support (ACLS). The initial assessment of SARS-CoV-2, serial ECGs, and cardiac markers are essential for a prompt approach and therapy in COVID-19-induced myocarditis.
Keywords: coronavirus; fulminant myocarditis; myocarditis; sars-cov-2; sudden death.
Copyright © 2022, Rodriguez Guerra et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Viral myocarditis—from pathophysiology to treatment. Schultheiss HP, Baumeier C, Aleshcheva G, Bock CT, Escher F. https://doi.org/10.3390/jcm10225240. J Clin Med. 2021;10:5240. - PMC - PubMed
-
- Myocarditis and inflammatory cardiomyopathy: current evidence and future directions. Tschöpe C, Ammirati E, Bozkurt B, et al. https://doi.org/10.1038/s41569-020-00435-x. Nat Rev Cardiol. 2021;18:169–193. - PMC - PubMed
-
- Clinically suspected myocarditis in the course of severe acute respiratory syndrome novel coronavirus-2 infection: fact or fiction? Ozieranski K, Tyminska A, Jonik S, et al. https://doi.org/10.1016/j.cardfail.2020.11.002. J Card Fail. 2021;27:92–96. - PMC - PubMed
-
- Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Caforio A L, Pankuweit S, Arbustini E et, al. al. https://pubmed.ncbi.nlm.nih.gov/23824828/ Eur Heart J. 2013;34:2636–2648. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous