

Contribution of Clinical Metagenomics to the Diagnosis of Bone and Joint Infections
- PMID: 35531285
- PMCID: PMC9069157
- DOI: 10.3389/fmicb.2022.863777
Contribution of Clinical Metagenomics to the Diagnosis of Bone and Joint Infections
Abstract
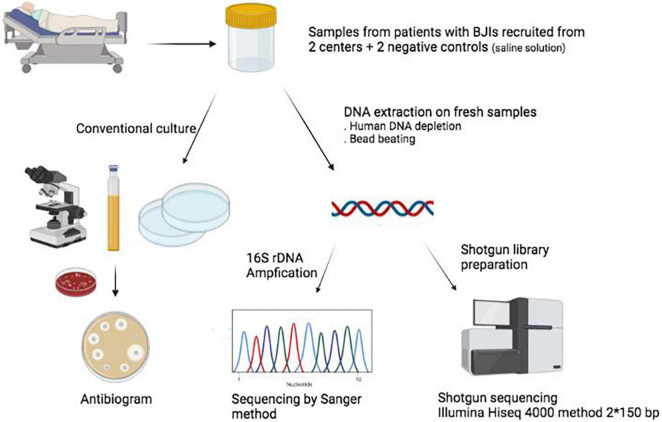
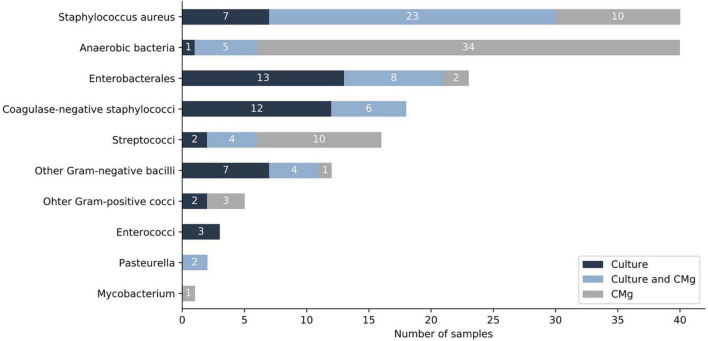
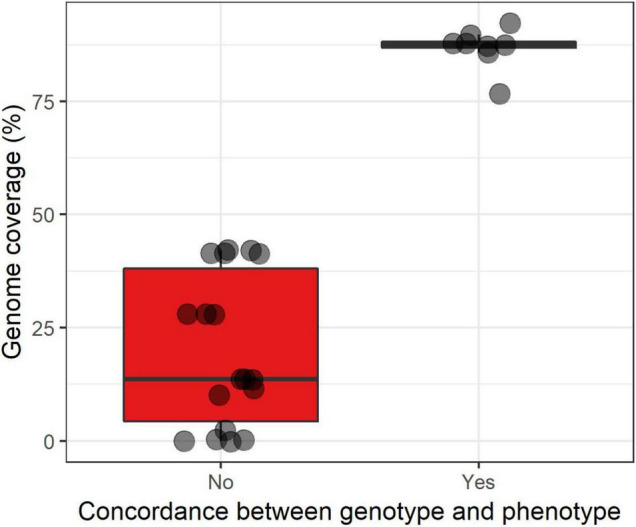
Bone and joint infections (BJIs) are complex infections that require precise microbiological documentation to optimize antibiotic therapy. Currently, diagnosis is based on microbiological culture, sometimes complemented by amplification and sequencing of the 16S rDNA gene. Clinical metagenomics (CMg), that is, the sequencing of the entire nucleic acids in a sample, was previously shown to identify bacteria not detected by conventional methods, but its actual contribution to the diagnosis remains to be assessed, especially with regard to 16S rDNA sequencing. In the present study, we tested the performance of CMg in 34 patients (94 samples) with suspected BJIs, as compared to culture and 16S rDNA sequencing. A total of 94 samples from 34 patients with suspicion of BJIs, recruited from two sites, were analyzed by (i) conventional culture, (ii) 16S rDNA sequencing (Sanger method), and (iii) CMg (Illumina Technology). Two negative controls were also sequenced by CMg for contamination assessment. Based on the sequencing results of negative controls, 414 out of 539 (76.7%) bacterial species detected by CMg were considered as contaminants and 125 (23.2%) as truly present. For monomicrobial infections (13 patients), the sensitivity of CMg was 83.3% as compared to culture, and 100% as compared to 16S rDNA. For polymicrobial infections (13 patients), the sensitivity of CMg was 50% compared to culture, and 100% compared to 16S rDNA. For samples negative in culture (8 patients, 21 samples), CMg detected 11 bacteria in 10 samples from 5 different patients. In 5/34 patients, CMg brought a microbiological diagnosis where conventional methods failed, and in 16/34 patients, CMg provided additional information. Finally, 99 antibiotic resistance genes were detected in 24 patients (56 samples). Provided sufficient genome coverage (87.5%), a correct inference of antibiotic susceptibility was achieved in 8/8 bacteria (100%). In conclusion, our study demonstrated that the CMg provides complementary and potentially valuable data to conventional methods of BJIs diagnosis.
Keywords: 16S rDNA gene analysis; Illumina; bone and joint infections; clinical metagenomics; diagnosis.
Copyright © 2022 d’Humières, Gaïa, Gueye, de Lastours, Leflon-Guibout, Maataoui, Duprilot, Lecronier, Rousseau, Gamany, Lescure, Senard, Deconinck, Dollat, Isernia, Le Hur, Petitjean, Nazimoudine, Le Gac, Chalal, Ferreira, Lazarevic, Guigon, Gervasi, Armand-Lefèvre, Schrenzel and Ruppé.
Conflict of interest statement
GGu and GGe were employed by bioMérieux SA. SF was employed by Genoscreen. ER received consulting fees from Illumina and Pathoquest. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources