

Population Attributable Fractions of Underlying Medical Conditions for Coronavirus Disease 2019 (COVID-19) Diagnosis and COVID-19 Hospitalizations, Ventilations, and Deaths Among Adults in the United States
- PMID: 35531382
- PMCID: PMC8992235
- DOI: 10.1093/ofid/ofac099
Population Attributable Fractions of Underlying Medical Conditions for Coronavirus Disease 2019 (COVID-19) Diagnosis and COVID-19 Hospitalizations, Ventilations, and Deaths Among Adults in the United States
Abstract
Background: Several underlying medical conditions have been reported to be associated with an increased risk of coronavirus disease 2019 (COVID-19) and related hospitalization and death. Population attributable fractions (PAFs) describing the proportion of disease burden attributable to underlying medical conditions for COVID-19 diagnosis and outcomes have not been reported.
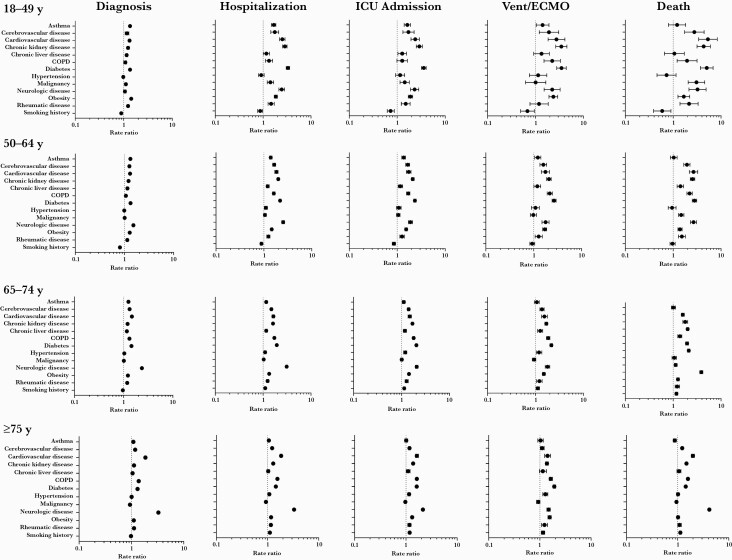
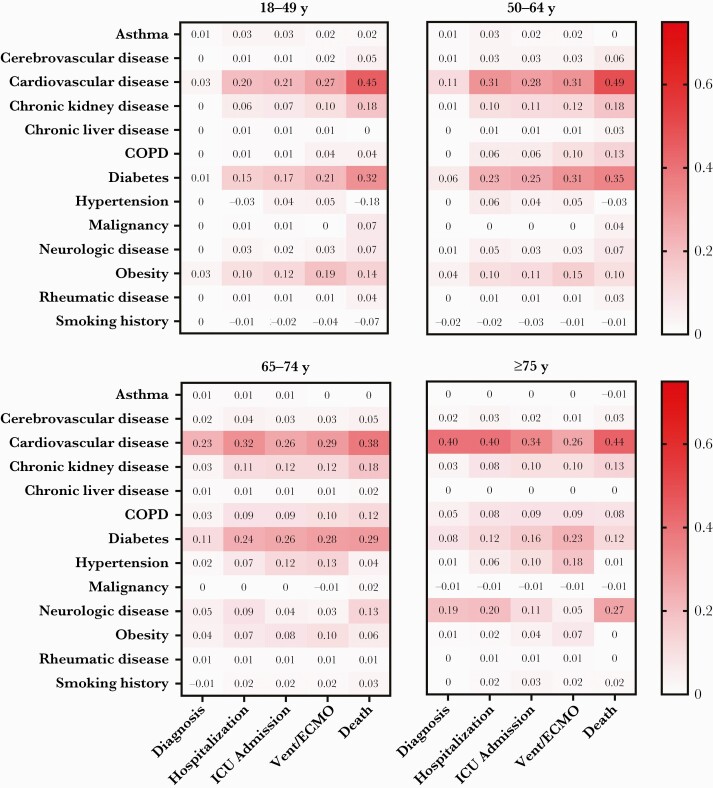
Methods: A retrospective population-based cohort study was conducted using Optum's de-identified Clinformatics Data Mart database. Individuals were followed up from 20 January 2020 to 31 December 2020 for diagnosis and clinical progression, including hospitalization, intensive care unit admission, intubation and mechanical ventilation or extracorporeal membrane oxygenation, and death. Adjusted rate ratios and PAFs of underlying medical conditions for COVID-19 diagnosis and disease progression outcomes were estimated by age (18-49, 50-64, 65-74, or ≥75 years), sex, and race/ethnicity.
Results: Of 10 679 566 cohort members, 391 964 (3.7%) were diagnosed with COVID-19, of whom 87 526 (22.3%) were hospitalized. Of those hospitalized, 26 640 (30.4%) died. Overall, cardiovascular disease and diabetes had the highest PAFs for COVID-19 diagnosis and outcomes of increasing severity across age groups (up to 0.49 and 0.35, respectively). Among adults ≥75 years of age, neurologic disease had the second-highest PAFs (0.05‒0.27) after cardiovascular disease (0.26‒0.44). PAFs were generally higher in Black persons than in other race/ethnicity groups for the same conditions, particularly in the 2 younger age groups.
Conclusions: A substantial fraction of the COVID-19 disease burden in the United States is attributable to cardiovascular disease and diabetes, highlighting the continued importance of COVID-19 prevention ( eg, vaccination, mask wearing, social distancing) and disease management of patients with certain underlying medical conditions.
Keywords: COVID-19; SARS-CoV-2; population attributable fraction; progression outcomes.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- World Health Organization. Coronavirus disease (COVID-19) dashboard. https://covid19.who.int/. Accessed 9 February 2022.
-
- Jordan RE, Adab P, Cheng KK.. COVID-19: risk factors for severe disease and death. BMJ 2020; 368:m1198. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
