

First report from the German COVID-19 autopsy registry
- PMID: 35531493
- PMCID: PMC9073019
- DOI: 10.1016/j.lanepe.2022.100330
First report from the German COVID-19 autopsy registry
Abstract
Background: Autopsies are an important tool in medicine, dissecting disease pathophysiology and causes of death. In COVID-19, autopsies revealed e.g., the effects on pulmonary (micro)vasculature or the nervous system, systemic viral spread, or the interplay with the immune system. To facilitate multicentre autopsy-based studies and provide a central hub supporting autopsy centres, researchers, and data analyses and reporting, in April 2020 the German COVID-19 Autopsy Registry (DeRegCOVID) was launched.
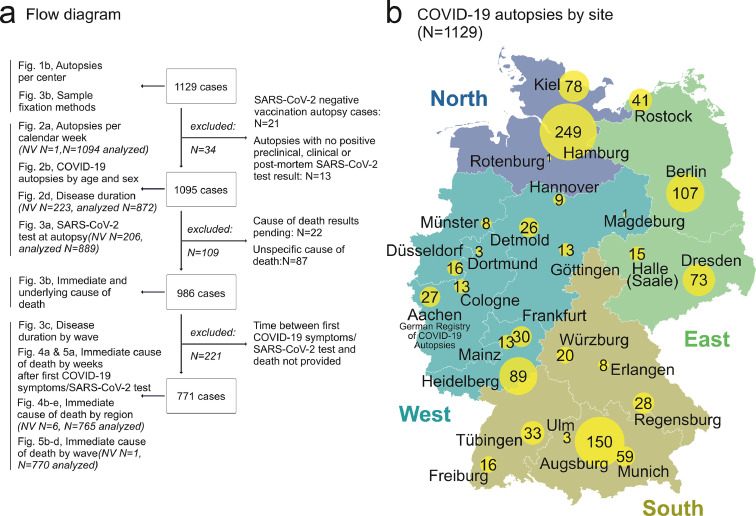
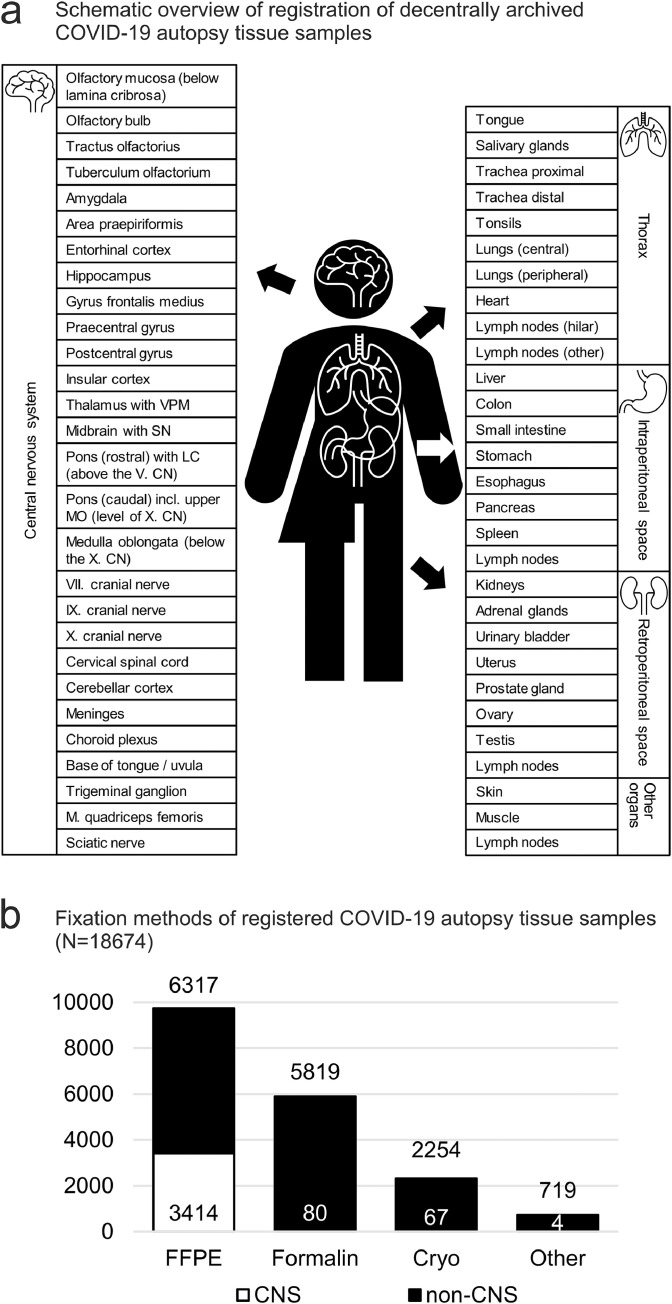
Methods: The electronic registry uses a web-based electronic case report form. Participation is voluntary and biomaterial remains at the respective site (decentralized biobanking). As of October 2021, the registry included N=1129 autopsy cases, with 69271 single data points including information on 18674 available biospecimens gathered from 29 German sites.
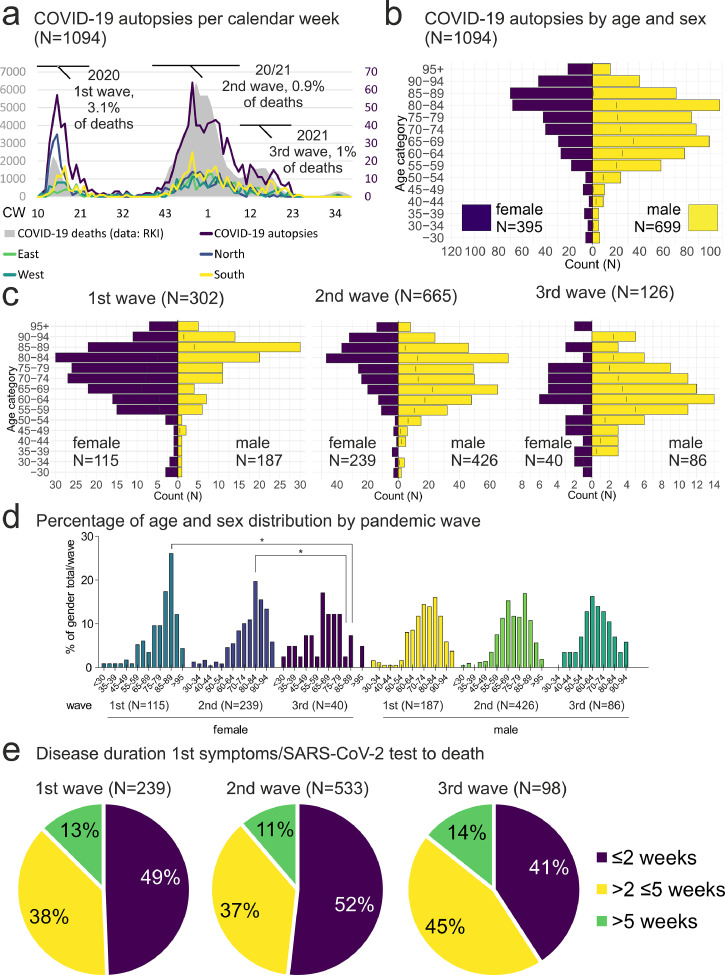
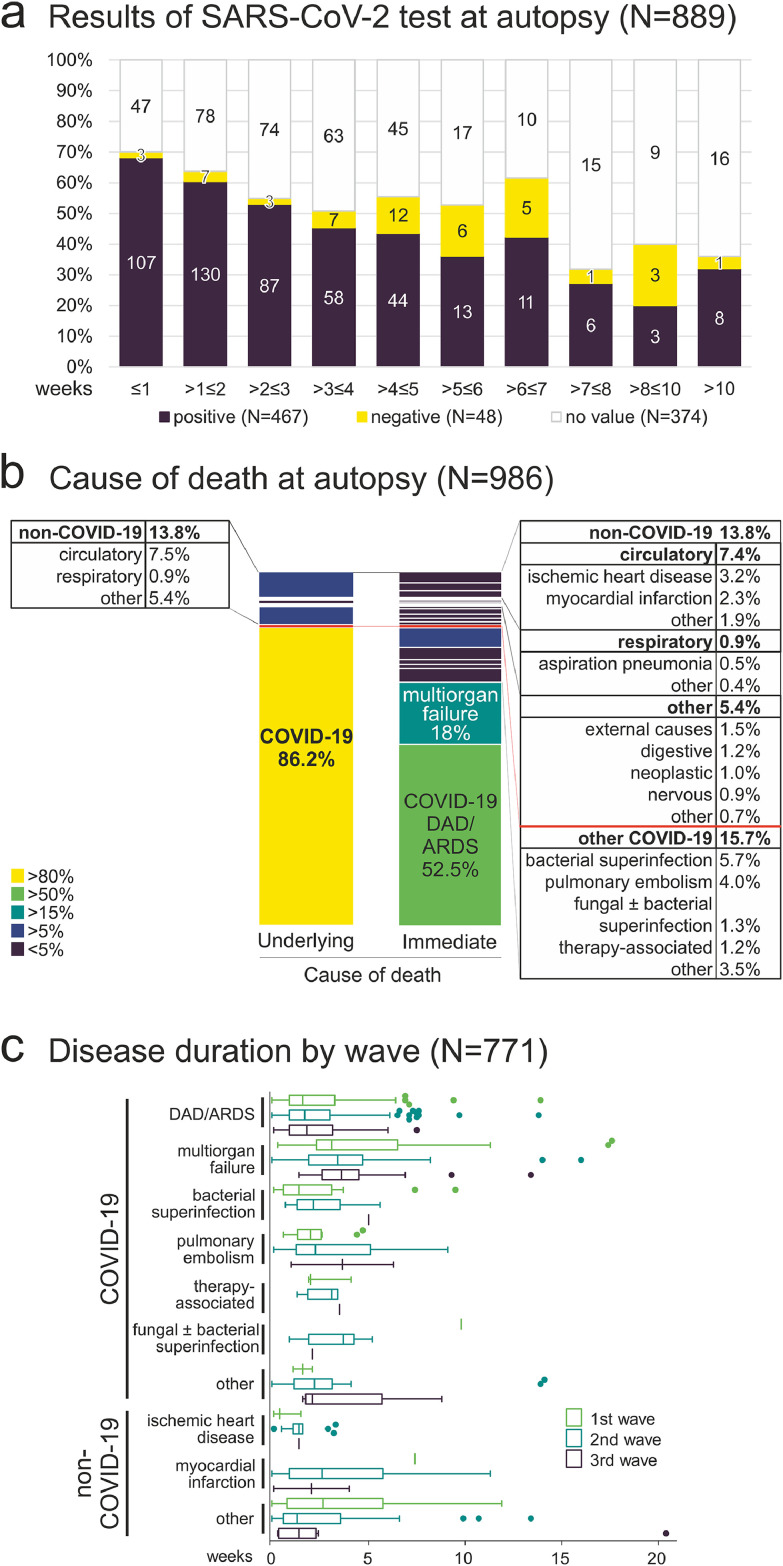
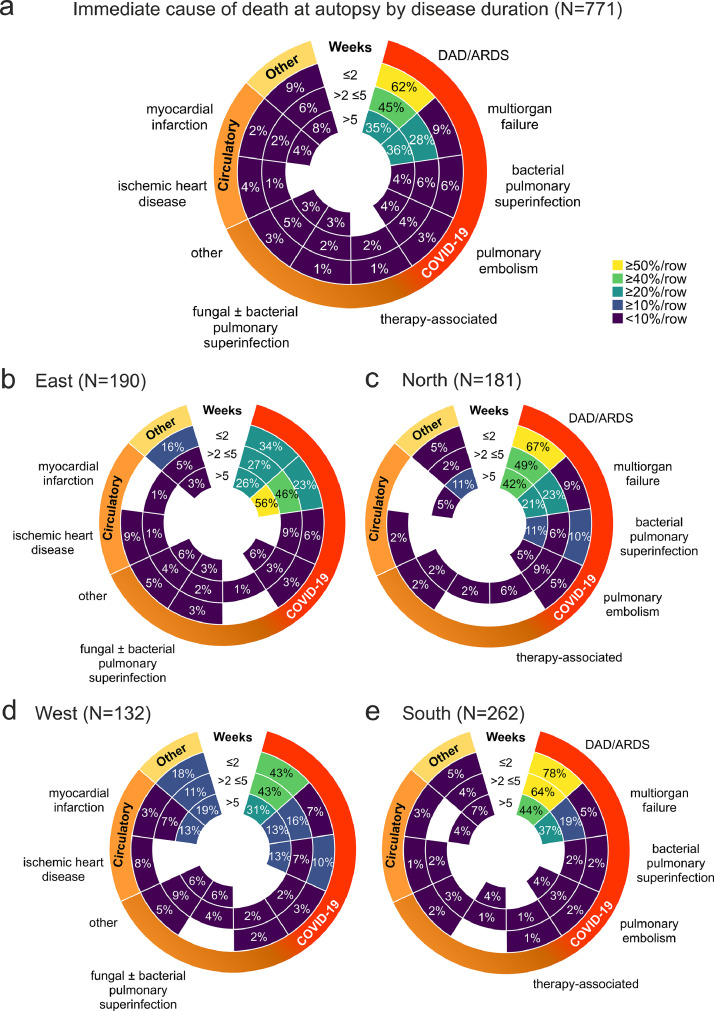
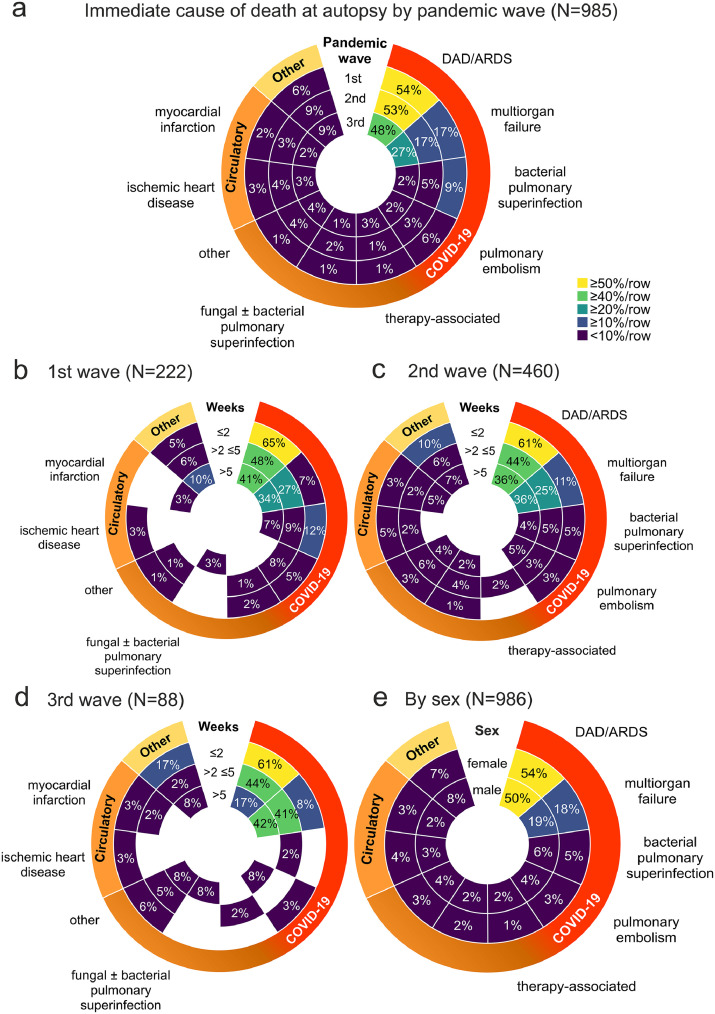
Findings: In the N=1095 eligible records, the male-to-female ratio was 1·8:1, with peaks at 65-69 and 80-84 years in males and >85 years in females. The analysis of the chain of events directly leading to death revealed COVID-19 as the underlying cause of death in 86% of the autopsy cases, whereas in 14% COVID-19 was a concomitant disease. The most common immediate cause of death was diffuse alveolar damage, followed by multi-organ failure. The registry supports several scientific projects, public outreach and provides reports to the federal health authorities, leading to legislative adaptation of the German Infection Protection Act, facilitating the performance of autopsies during pandemics.
Interpretation: A national autopsy registry can provide multicentre quantitative information on COVID-19 deaths on a national level, supporting medical research, political decision-making and public discussion.
Funding: German Federal Ministries of Education and Research and Health.Hintergrund: Obduktionen sind ein wichtiges Instrument in der Medizin, um die Pathophysiologie von Krankheiten und Todesursachen zu untersuchen. Im Rahmen von COVID-19 wurden durch Obduktionen z.B. die Auswirkungen auf die pulmonale Mikrovaskulatur, das Nervensystem, die systemische Virusausbreitung, und das Zusammenspiel mit dem Immunsystem untersucht. Um multizentrische, auf Obduktionen basierende Studien zu erleichtern und eine zentrale Anlaufstelle zu schaffen, die Obduktionszentren, Forscher sowie Datenanalysen und -berichte unterstützt, wurde im April 2020 das deutsche COVID-19-Autopsieregister (DeRegCOVID) ins Leben gerufen.Methoden: Das elektronische Register verwendet ein webbasiertes elektronisches Fallberichtsformular. Die Teilnahme ist freiwillig und das Biomaterial verbleibt am jeweiligen Standort (dezentrales Biobanking). Im Oktober 2021 umfasste das Register N=1129 Obduktionsfälle mit 69271 einzelnen Datenpunkten, die Informationen über 18674 verfügbare Bioproben enthielten, die von 29 deutschen Standorten gesammelt wurden.Ergebnisse: In den N=1095 ausgewerteten Datensätzen betrug das Verhältnis von Männern zu Frauen 1,8:1 mit Spitzenwerten bei 65-69 und 80-84 Jahren bei Männern und >85 Jahren bei Frauen. Die Analyse der Sequenz der unmittelbar zum Tod führenden Ereignisse ergab, dass in 86 % der Obduktionsfälle COVID-19 die zugrunde liegende Todesursache war, während in 14 % der Fälle COVID-19 eine Begleiterkrankung war. Die häufigste unmittelbare Todesursache war der diffuse Alveolarschaden, gefolgt von Multiorganversagen. Das Register unterstützt mehrere wissenschaftliche Projekte, die Öffentlichkeitsarbeit und liefert Berichte an die Bundesgesundheitsbehörden, was zu einer Anpassung des deutschen Infektionsschutzgesetzes führte und die Durchführung von Obduktionen in Pandemien erleichtert.Interpretation: Ein nationales Obduktionsregister kann multizentrische quantitative Informationen über COVID-19-Todesfälle auf nationaler Ebene liefern und damit die medizinische Forschung, die politische Entscheidungsfindung und die öffentliche Diskussion unterstützen.Finanzierung: Bundesministerien für Bildung und Forschung und für Gesundheit.
Keywords: Autopsy; COVID-19; Cause of Death; Registry; SARS-CoV-2.
© 2022 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Rybakova MG, Karev VE, Kuznetsova IA. [Anatomical pathology of novel coronavirus (COVID-19) infection. First impressions] Arkh Patol. 2020;82(5):5–15. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
