

Antroduodenal motility recording identifies characteristic patterns in gastroparesis related to underlying etiology
- PMID: 35531931
- PMCID: PMC9788094
- DOI: 10.1111/nmo.14394
Antroduodenal motility recording identifies characteristic patterns in gastroparesis related to underlying etiology
Abstract
Background: Gastroparesis (GP) is a gastrointestinal disorder associated with significant morbidity and healthcare costs. GP patients form a heterogeneous population with diverse etiology, and treatment is often challenging due to a poorly understood underlying pathophysiology. The aim of the present study was to assess antroduodenal motility patterns among the different GP etiologies.
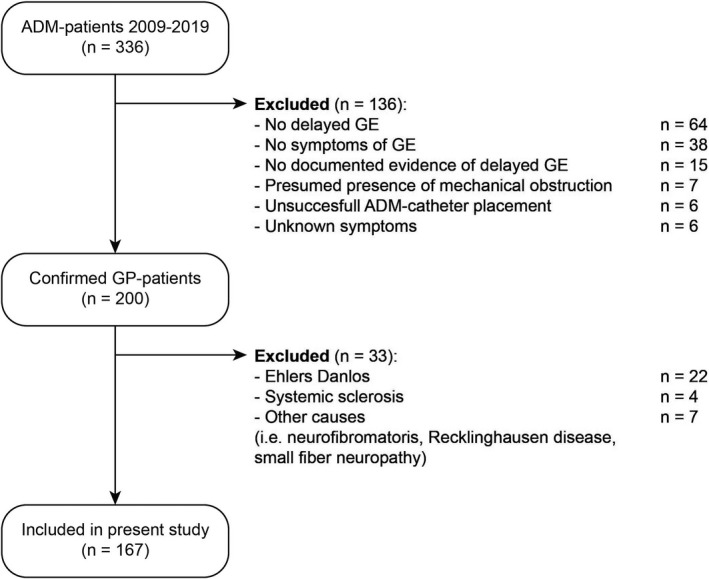
Methods: We reviewed antroduodenal manometry (ADM) recordings of patients with confirmed GP between 2009 and 2019. ADM measurements were evaluated for fed period duration, number of phase III contractions and migrating motor complexes (MMCs), motility index (MI), and presence of neuropathic patterns.
Key results: A total of 167 GP patients (142 women, median age 45 [31-57]) were included. The following etiologies were identified: idiopathic n = 101; post-surgery n = 36; and diabetes n = 30. Fed period duration was significantly longer in idiopathic (p < 0.01) and diabetic GP patients (p < 0.05) compared with post-surgery GP patients. Furthermore, the number and duration of phase III contractions and the number of MMCs were significantly lower in idiopathic and diabetic patients compared with post-surgery GP patients (p < 0.01). Likewise, absence of MMCs during 6-h recording was more often observed in idiopathic and diabetes GP patients compared with post-surgery GP patients (resp. p < 0.01 and p < 0.05).
Conclusions and inferences: Antroduodenal motility patterns are different among GP etiologies. A dysmotility spectrum was identified with different patterns ranging from post-surgery GP to idiopathic and diabetic GP.
Keywords: antroduodenal manometry; gastrointestinal motility; gastroparesis; migrating motor complex.
© 2022 The Authors. Neurogastroenterology & Motility published by John Wiley & Sons Ltd.
Conflict of interest statement
All authors declare no conflict of interests.
Figures




References
-
- Parkman HP, Hasler WL, Fisher RS, American Gastroenterological A . American Gastroenterological Association medical position statement: diagnosis and treatment of gastroparesis. Gastroenterology. 2004;127(5):1589‐1591. - PubMed
-
- Lacy BE, Crowell MD, Mathis C, Bauer D, Heinberg LJ. Gastroparesis: quality of life and health care utilization. J Clin Gastroenterol. 2018;52(1):20‐24. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
