

Current concept of kinematic alignment total knee arthroplasty and its derivatives
- PMID: 35532356
- PMCID: PMC9134837
- DOI: 10.1302/2633-1462.35.BJO-2022-0021.R2
Current concept of kinematic alignment total knee arthroplasty and its derivatives
Abstract
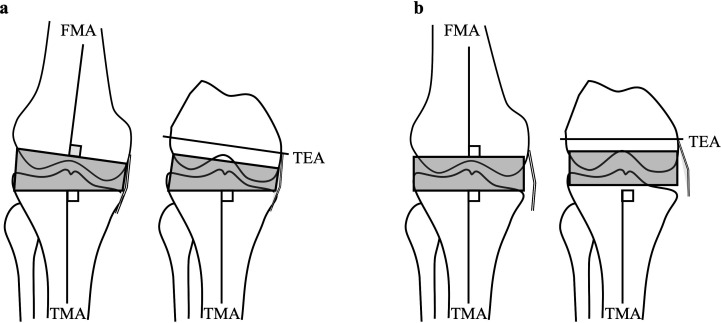
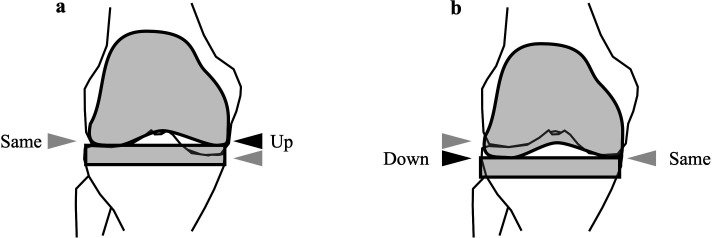
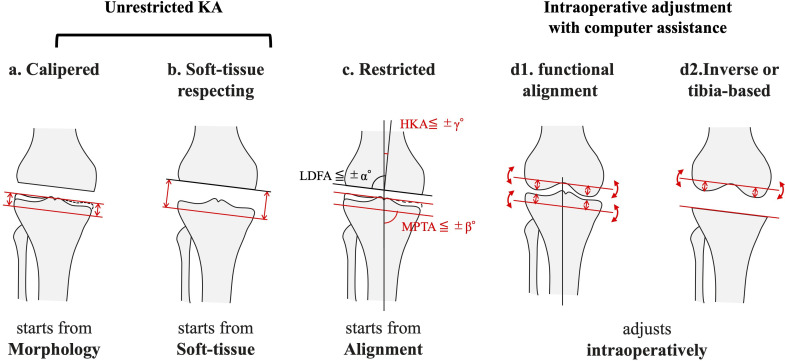
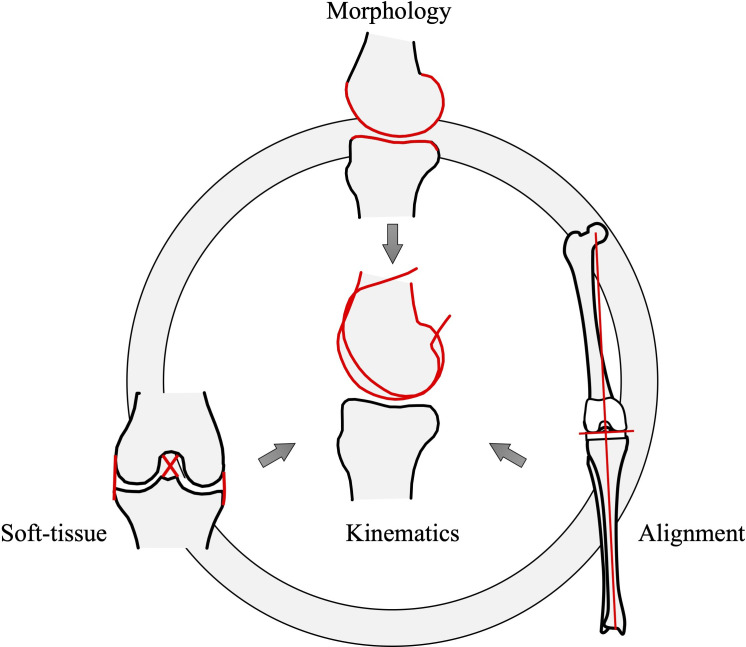
The kinematic alignment (KA) approach to total knee arthroplasty (TKA) has recently increased in popularity. Accordingly, a number of derivatives have arisen and have caused confusion. Clarification is therefore needed for a better understanding of KA-TKA. Calipered (or true, pure) KA is performed by cutting the bone parallel to the articular surface, compensating for cartilage wear. In soft-tissue respecting KA, the tibial cutting surface is decided parallel to the femoral cutting surface (or trial component) with in-line traction. These approaches are categorized as unrestricted KA because there is no consideration of leg alignment or component orientation. Restricted KA is an approach where the periarthritic joint surface is replicated within a safe range, due to concerns about extreme alignments that have been considered 'alignment outliers' in the neutral mechanical alignment approach. More recently, functional alignment and inverse kinematic alignment have been advocated, where bone cuts are made following intraoperative planning, using intraoperative measurements acquired with computer assistance to fulfill good coordination of soft-tissue balance and alignment. The KA-TKA approach aims to restore the patients' own harmony of three knee elements (morphology, soft-tissue balance, and alignment) and eventually the patients' own kinematics. The respective approaches start from different points corresponding to one of the elements, yet each aim for the same goal, although the existing implants and techniques have not yet perfectly fulfilled that goal.
Keywords: Alignment; Arthroplasty; Kinematic; Knee; Mechanical; Soft-tissue; Treatment; cartilage; femur; kinematics; knees; soft-tissue; soft-tissue balancing; tibial bone; tibial components; tibial cutting; total knee arthroplasty (TKA).
Figures
Similar articles
-
Current concept: personalized alignment total knee arthroplasty as a contrast to classical mechanical alignment total knee arthroplasty.Arthroplasty. 2024 May 6;6(1):23. doi: 10.1186/s42836-024-00246-2. Arthroplasty. 2024. PMID: 38705976 Free PMC article.
-
Deviations in femoral joint lines using calipered kinematically aligned TKA from virtually planned joint lines are small and do not affect clinical outcomes.Knee Surg Sports Traumatol Arthrosc. 2020 Oct;28(10):3118-3127. doi: 10.1007/s00167-019-05776-w. Epub 2019 Nov 25. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 31768572
-
Kinematically Aligned Total Knee Arthroplasty Using Calipered Measurements, Manual Instruments, and Verification Checks.2020 Jul 1. In: Rivière C, Vendittoli PA, editors. Personalized Hip and Knee Joint Replacement [Internet]. Cham (CH): Springer; 2020. Chapter 24. 2020 Jul 1. In: Rivière C, Vendittoli PA, editors. Personalized Hip and Knee Joint Replacement [Internet]. Cham (CH): Springer; 2020. Chapter 24. PMID: 33347137 Free Books & Documents. Review.
-
Personalized alignment in total knee arthroplasty: current concepts.SICOT J. 2021;7:19. doi: 10.1051/sicotj/2021021. Epub 2021 Mar 26. SICOT J. 2021. PMID: 33812467 Free PMC article.
-
Kinematic alignment of medial UKA is safe: a systematic review.Knee Surg Sports Traumatol Arthrosc. 2022 Mar;30(3):1082-1094. doi: 10.1007/s00167-021-06462-6. Epub 2021 Mar 20. Knee Surg Sports Traumatol Arthrosc. 2022. PMID: 33743031
Cited by
-
Current concept: personalized alignment total knee arthroplasty as a contrast to classical mechanical alignment total knee arthroplasty.Arthroplasty. 2024 May 6;6(1):23. doi: 10.1186/s42836-024-00246-2. Arthroplasty. 2024. PMID: 38705976 Free PMC article.
-
Postoperative clinical outcomes for kinematically, restricted kinematically, or mechanically aligned total knee arthroplasty: a systematic review and network meta-analysis of randomized controlled trials.BMC Musculoskelet Disord. 2023 Apr 24;24(1):322. doi: 10.1186/s12891-023-06448-0. BMC Musculoskelet Disord. 2023. PMID: 37095485 Free PMC article.
-
Systematic review and meta-analysis of long term outcomes and innovations in Total Knee Arthroplasty: KINEMATIC, PERSONALIZED KNEE vs. CONVENTIONAL.Orthop Rev (Pavia). 2024 Aug 29;16:122318. doi: 10.52965/001c.122318. eCollection 2024. Orthop Rev (Pavia). 2024. PMID: 39219731 Free PMC article.
-
Effects of Unrestricted Kinematically Aligned Total Knee Arthroplasty with a Modified Soft-Tissue Respecting Technique on the Deformity of Limb Alignment in Japanese Patients.Medicina (Kaunas). 2023 Nov 8;59(11):1969. doi: 10.3390/medicina59111969. Medicina (Kaunas). 2023. PMID: 38004019 Free PMC article.
-
Addressing sagittal plane imbalance in primary total knee arthroplasty.Bone Jt Open. 2024 Aug 19;5(8):681-687. doi: 10.1302/2633-1462.58.BJO-2024-0040.R1. Bone Jt Open. 2024. PMID: 39155644 Free PMC article.
References
-
- No authors listed . NJR 17th Annual Report 2020. National Joint Registry. 2021. https://reports.njrcentre.org.uk/Portals/0/PDFdownloads/NJR%2017th%20Ann... (date last accessed 1 April 2022).
-
- No authors listed . Australian Orthopaedic Association National Joint Replacement Registry 20th Annual Report 2020. Australian Orthopaedic Association National Joint Replacement Registry. 2020. https://aoanjrr.sahmri.com/documents/10180/668596/Hip%2C+Knee+%26+Should... (date last accessed 1 April 2022).
-
- No authors listed . The New Zealand Joint Registry twenty-one year report January 1999 to December 2019. New Zealand Orthopaedic Association. 2020. https://nzoa.org.nz/sites/default/files/DH8426_NZJR_2020_Report_v5_30Sep... (date last accessed 1 April 2022).
LinkOut - more resources
Full Text Sources
Medical
