

Full Reperfusion Without Functional Independence After Mechanical Thrombectomy in the Anterior Circulation : Performance of Prediction Models Before Versus After Treatment Initiation
- PMID: 35532751
- PMCID: PMC9744692
- DOI: 10.1007/s00062-022-01166-x
Full Reperfusion Without Functional Independence After Mechanical Thrombectomy in the Anterior Circulation : Performance of Prediction Models Before Versus After Treatment Initiation
Abstract
Background and purpose: Prediction of futile recanalization (FR), i.e. failure of long-term functional independence despite full reperfusion in mechanical thrombectomy (MT), is instrumental in patients undergoing endovascular therapy.
Methods: Retrospective single-center analysis of patients treated for anterior circulation LVO ensuing successful MT (mTICI 2c-3) between January 2014 and April 2019. FR was defined as modified Rankin Scale (mRS) 90 days after stroke onset > 2 or mRS > pre-stroke mRS. Multivariable analysis was performed with variables available before treatment initiation regarding their association with FR. Performance of the regression model was then compared with a model including parameters available after MT.
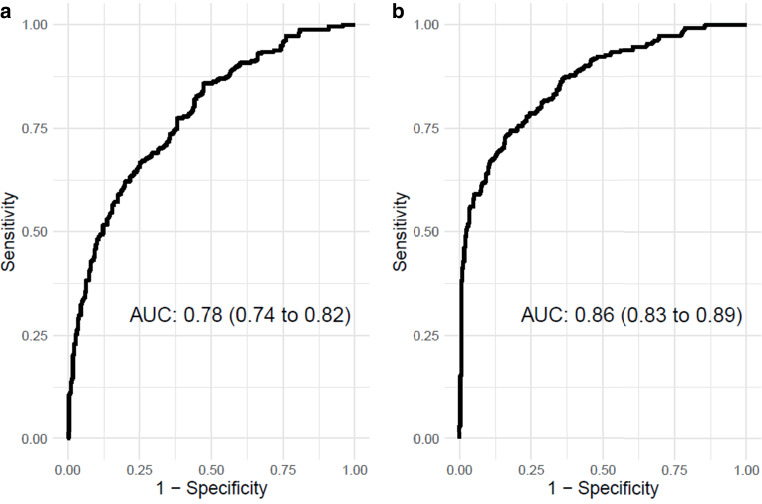
Results: Successful MT was experienced by 549/1146 patients in total. FR occurred in 262/549 (47.7%) patients. Independent predictors of FR were male sex, odds ratio (OR) with 95% confidence interval (CI) 1.98 (1.31-3.05, p 0.001), age (OR 1.05, CI 1.03-1.07, p < 0.001), NIHSS on admission (OR 1.10, CI 1.06-1.13, p < 0.001), pre-stroke mRS (OR 1.22, CI 1.03-1.46, p 0.025), neutrophile-lymphocyte ratio (OR 1.03, CI 1.00-1.06, p 0.022), baseline ASPECTS (OR 0.77, CI 0.68-0.88, p < 0.001), and absence of bridging i.v. lysis (OR 1.62, 1.09-2.42, p 0.016). The prediction model's Area Under the Curve was 0.78 (CI 0.74-0.82) and increased with parameters available after MT to 0.86 (CI 0.83-0.89) with failure of early neurological improvement being the most important predictor of FR (OR 15.0, CI 7.2-33.8).
Conclusion: A variety of preinterventional factors may predict FR with substantial certainty, but the prediction model can still be improved by considering parameters only available after MT, in particular early neurological improvement.
Keywords: Early neurological improvement; Futile recanalization; Ischemic stroke; Logistic regression models; Outcome prediction.
© 2022. The Author(s).
Conflict of interest statement
All authors declare that there is no conflict of interest related to the submitted study and manuscript. Disclosures: C. S. Weyland—none. J. A. Vey—none. Y. Mokli—none. M. Feisst—none. M. Kieser—none. C. Herweh—UNRELATED: Consultancy: Brainomix, Oxford, UK. S. Schönenberger—none. M. Bendszus—UNRELATED: Grants from Siemens, grants and personal fees from Novartis, grants from Stryker, grants from DFG, personal fees from Merck, personal fees from Bayer, personal fees from Teva, grants and personal fees from Guerbet, personalfees from Boehringer, personal fees from Vascular Dynamics, personal fees from Grifols, and grants from European Union, all outside the submitted work. M. A. Möhlenbruch—UNRELATED: Board Membership: Codman; Consultancy: Medtronic, MicroVention, Stryker; Payment for Lectures Including Service on Speakers Bureaus: Medtronic, MicroVention, Stryker. *Money paid to the institution. P. A. Ringleb—UNRELATED: Consultancy: Boehringer, Lecture fees from Bayer, Boehringer Ingelheim, BMS, Daichii Sankyo, Pfizer. S. Nagel—UNRELATED: Consultancy: Brainomix, Boehringer Ingelheim; Payment for Lectures Including Service on Speakers Bureaus: Pfizer, Medtronic, Bayer AG.
Figures
Similar articles
-
Predictors of futile recanalization in ischemic stroke patients with low baseline NIHSS.Int J Stroke. 2024 Dec;19(10):1102-1112. doi: 10.1177/17474930241264737. Epub 2024 Nov 19. Int J Stroke. 2024. PMID: 38888031 Free PMC article.
-
Stress hyperglycemia as a modifiable predictor of futile recanalization in patients undergoing mechanical thrombectomy for acute ischemic stroke.Front Neurol. 2023 May 19;14:1170215. doi: 10.3389/fneur.2023.1170215. eCollection 2023. Front Neurol. 2023. PMID: 37273693 Free PMC article.
-
Predictive factors of functional independence after optimal reperfusion in anterior circulation ischaemic stroke with indication for intravenous thrombolysis plus mechanical thrombectomy.Eur J Neurol. 2021 Jan;28(1):141-151. doi: 10.1111/ene.14509. Epub 2020 Oct 13. Eur J Neurol. 2021. PMID: 32916042
-
Cystatin C predicts futile recanalization in patients with acute ischemic stroke after endovascular treatment.J Neurol. 2022 Feb;269(2):966-972. doi: 10.1007/s00415-021-10680-w. Epub 2021 Jul 5. J Neurol. 2022. PMID: 34226965
-
Mechanical Thrombectomy vs Bridging Therapy for Anterior Circulation Large Vessel Occlusion Stroke: Systematic Review and Meta-analysis.Neurology. 2022 Mar 29;98(13):e1361-e1373. doi: 10.1212/WNL.0000000000200029. Epub 2022 Feb 16. Neurology. 2022. PMID: 35173017
Cited by
-
Prognostic role of dynamic neutrophil-to-lymphocyte ratio in acute ischemic stroke after reperfusion therapy: A meta-analysis.Front Neurol. 2023 Feb 16;14:1118563. doi: 10.3389/fneur.2023.1118563. eCollection 2023. Front Neurol. 2023. PMID: 36873451 Free PMC article.
-
Association Between Early Spontaneous Post-Thrombectomy Blood Pressure Reduction and Clinical Outcomes in Large Vessel Occlusion Stroke.Brain Behav. 2025 Jul;15(7):e70677. doi: 10.1002/brb3.70677. Brain Behav. 2025. PMID: 40621714 Free PMC article.
-
Age-Specific Differences in Inflammatory Biomarkers and Their Impact on Futile Recanalization After Mechanical Thrombectomy: An Inverse Probability Weighting Analysis.Eur J Neurol. 2025 May;32(5):e70182. doi: 10.1111/ene.70182. Eur J Neurol. 2025. PMID: 40353608 Free PMC article.
-
Development and Validation of a Postprocedural Model to Predict Outcome After Endovascular Treatment for Ischemic Stroke.JAMA Neurol. 2023 Jul 31;80(9):940-8. doi: 10.1001/jamaneurol.2023.2392. Online ahead of print. JAMA Neurol. 2023. PMID: 37523199 Free PMC article.
-
Modified treatment in cerebral ischemia 1 versus modified treatment in cerebral ischemia 0 before endovascular stroke treatment in middle cerebral artery's M1-occlusion: Predictor for revascularization success and outcome?Interv Neuroradiol. 2025 Apr;31(2):195-200. doi: 10.1177/15910199231155297. Epub 2023 Feb 21. Interv Neuroradiol. 2025. PMID: 40260698 Free PMC article.
References
-
- Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, Davalos A, Majoie CB, van der Lugt A, de Miquel MA, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387:1723–1731. doi: 10.1016/S0140-6736(16)00163-X. - DOI - PubMed
-
- Adams HP, Jr., Davis PH, Leira EC, Chang KC, Bendixen BH, Clarke WR, Woolson RF, Hansen MD. Baseline NIH stroke scale score strongly predicts outcome after stroke: a report of the trial of Org 10172 in acute stroke treatment (TOAST) Neurology. 1999;53:126–131. doi: 10.1212/WNL.53.1.126. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
