

Clinical benefit and cost-effectiveness analysis of liquid biopsy application in patients with advanced non-small cell lung cancer (NSCLC): a modelling approach
- PMID: 35532791
- PMCID: PMC10020305
- DOI: 10.1007/s00432-022-04034-w
Clinical benefit and cost-effectiveness analysis of liquid biopsy application in patients with advanced non-small cell lung cancer (NSCLC): a modelling approach
Abstract
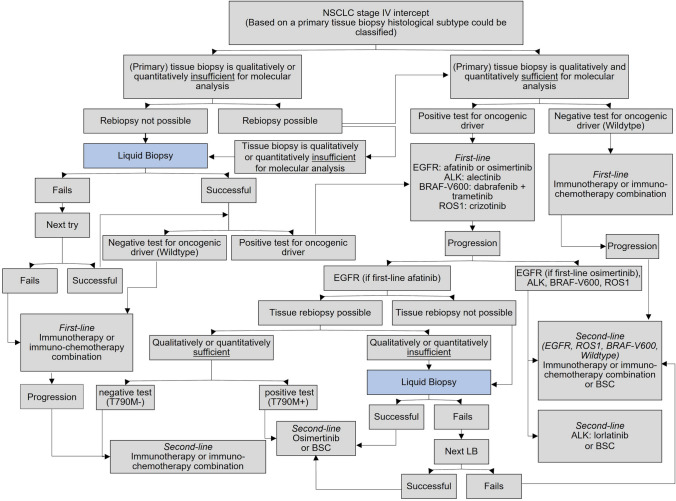
Purpose: Targeted therapies are effective therapeutic approaches in advanced stages of NSCLC and require precise molecular profiling to identify oncogenic drivers. Differential diagnosis on a molecular level contributes to clinical decision making. Liquid biopsy (LB) use has demonstrated its potential to serve as an alternative to tissue biopsy (TB) particularly in cases where tissue sampling is not feasible or insufficient. We aimed at evaluating the cost-effectiveness of ctDNA-based LB use (molecular multigene testing) according to German care guidelines for metastatic NSCLC.
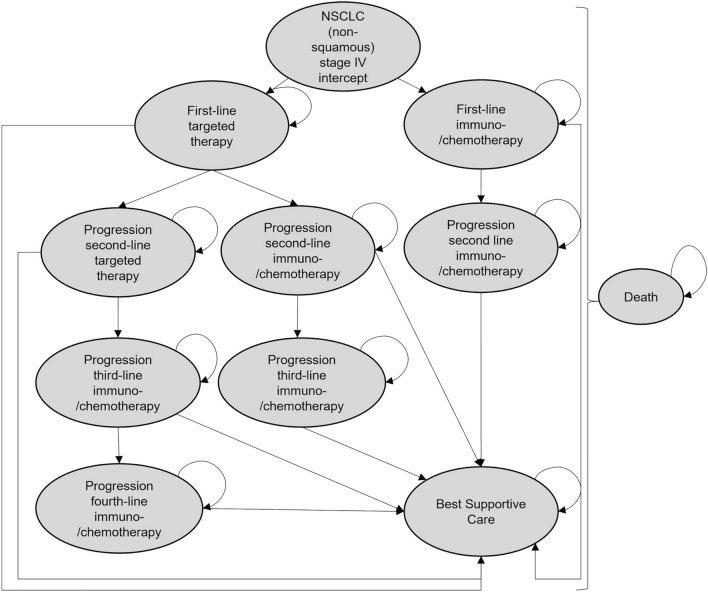
Methods: A Markov model was developed to compare the costs and clinical benefits associated with the use of LB as an add-on to TB according to the guidelines for NSCLC patients. Usual care TB served as comparator. A microsimulation model was used to simulate a cohort of non-squamous NSCLC patients stage IV. The parameters used for modelling were obtained from the literature and from the prospective German CRISP registry ("Clinical Research platform Into molecular testing, treatment, and outcome of non-Small cell lung carcinoma Patients"). For each pathway, average direct medical costs, and QALYs gained per patient were used for calculating incremental cost-effectiveness ratios (ICER).
Results: The use of LB as an add-on was costlier (€144,981 vs. €144,587) but more effective measured in QALYs (1.20 vs. 1.19) for the care pathway of NSCLC patients (ICER €53,909/QALY). Cost-effectiveness was shown for EGFR-mutated patients (ICER €-13,247/QALY).
Conclusion: Including LB as an add-on into the care pathway of advanced NSCLC has positive clinical effects in terms of QALYs accompanied by a moderate cost-effectiveness.
Keywords: Cost-effectiveness; Liquid biopsy; Molecular profiling; NSCLC.
© 2022. The Author(s).
Conflict of interest statement
Fabienne Englmeier and Klaus Nagels have received payments from Roche Pharma AG to their institution during the conduct of the study. Klaus Nagels reports personal fees from Amgen, Lilly, Roche, Novartis, outside the submitted work; Annalen Bleckmann reports personal fees from Alexion, Gilead, Novartis, BMS, Bayer, Servier, Roche, AstraZeneca, Takeda, Merck, Boehringer Ingelheim, Lilly Pharma, Abbvie, BeiGene outside the submitted work. Annalen Bleckmann participated on the Roche Advisory Board outside the submitted work; Wolfgang Brueckl reports personal fees from Astra Zeneca, BMS, Boehringer Ingelheim, MSD, Lilly Pharma, Pfizer, Roche, Chugai, Takeda, Novartis, outside the submitted work; Wolfgang Brueckl participated on several Advisory Boards (AstraZeneca, Boehringer Ingelheim, Novartis, MSD, Lilly Pharma, BMS, Roche), outside the submitted work. Frank Griesinger reports grants to the institution from AstraZeneca, Boehringer Ingelheim, BMS, Lilly Pharma, MSD, Novartis, Pfizer, Roche, Takeda, Siemens, AMGEN, GSK, Johnson & Johnson, outside the submitted work. Frank Griesinger reports personal fees from Advisory Board Roche, Boehringer Ingelheim, Takeda, Abbvie, AstraZeneca, MSD, Pfizer, Sobi, Merck, Bristol-Myers Squibb, Janssen-Cilag, AMGEN, Ipsen, Novartis, outside the submitted work. Frank Griesinger participated on several Advisory Boards (Roche, Boehringer Ingelheim, Takeda, Abbvie, AstraZeneca, MSD, Pfizer, Sobi, Merck, Bristol-Myers Squibb, Janssen-Cilag, AMGEN, Ipsen, Novartis), outside the submitted work. Annette Fleitz declares that she has no conflicts of interests.
Figures





References
-
- AIO, iOMedico (2021) CRISP register platform lung cancer (AIO-TRK-0315): special analysis database cut 30.06.2020 (unpublished data)
-
- Aktuell DKG (2020) Positionspapier–Testung in der Onkologie. Forum 35:268–273. 10.1007/s12312-020-00831-x
-
- Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e. V (2018) S3-Leitlinie: Prävention, Diagnostik, Therapie und Nachsorge des Lungenkarzinoms. http://leitlinienprogramm-on-kologie.de/Lungenkarzinom.98.0.html. Accessed 2 March 2020
-
- Arcila ME, Oxnard GR, Nafa K, Riely GJ, Solomon SB, Zakowski MF, Kris MG, Pao W, Miller VA, Ladanyi M (2011) Rebiopsy of lung cancer patients with acquired resistance to EGFR inhibitors and enhanced detection of the T790M mutation using a locked nucleic acid-based assay. Clin Cancer Res 17:1169–1180. 10.1158/1078-0432.CCR-10-2277 - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
