

Prognostic value of stress hyperglycemia ratio on short- and long-term mortality after acute myocardial infarction
- PMID: 35532812
- PMCID: PMC9242951
- DOI: 10.1007/s00592-022-01893-0
Prognostic value of stress hyperglycemia ratio on short- and long-term mortality after acute myocardial infarction
Abstract
Aims: Prior studies demonstrated an association between hospital admission blood glucose and mortality in acute myocardial infarction (AMI). Because stress hyperglycemia ratio (SHR) has been suggested as a more reliable marker of stress hyperglycemia this study investigated to what extent SHR in comparison with admission blood glucose is associated with short- and long-term mortality in diabetic and non-diabetic AMI patients.
Methods: The analysis was based on 2,311 AMI patients aged 25-84 years from the population-based Myocardial Infarction Registry Augsburg (median follow-up time 6.5 years [IQR: 4.9-8.1]). The SHR was calculated as admission glucose (mg/dl)/(28.7 × HbA1c (%)-46.7). Using logistic and COX regression analyses the associations between SHR and admission glucose and mortality were investigated.
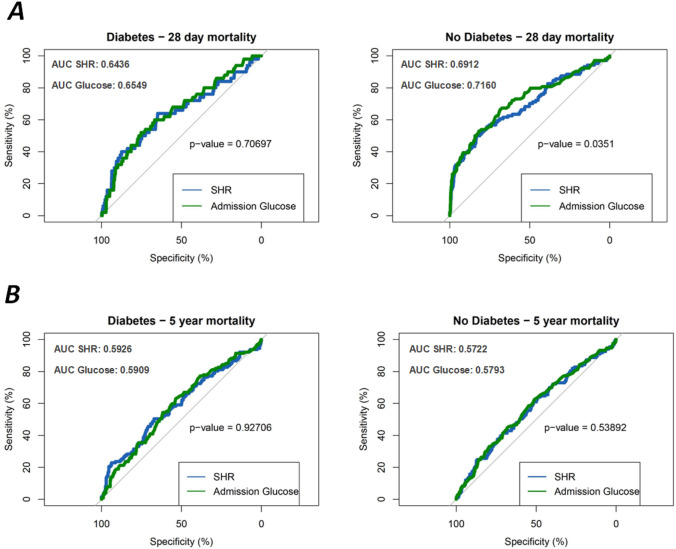
Result: Higher admission glucose and higher SHR were significantly and nonlinearly associated with higher 28-day mortality in AMI patients with and without diabetes. In patients without diabetes, the AUC for SHR was significantly lower than for admission glucose (SHR: 0.6912 [95%CI 0.6317-0.7496], admission glucose: 0.716 [95%CI 0.6572-0.7736], p-value: 0.0351). In patients with diabetes the AUCs were similar for SHR and admission glucose. Increasing admission glucose and SHR were significantly nonlinearly associated with higher 5-year all-cause mortality in AMI patients with diabetes but not in non-diabetic patients. AUC values indicated a comparable prediction of 5-year mortality for both measures in diabetic and non-diabetic patients.
Conclusions: Stress hyperglycemia in AMI patients plays a significant role mainly with regard to short-term prognosis, but barely so for long-term prognosis, underlining the assumption that it is a transient dynamic disorder that occurs to varying degrees during the acute event, thereby affecting prognosis.
Keywords: Admission glucose; Long-term mortality; Myocardial infarction; Short-term mortality; Stress hyperglycemia.
© 2022. The Author(s).
Conflict of interest statement
None.
Figures



Similar articles
-
The impact of fasting stress hyperglycemia ratio, fasting plasma glucose and hemoglobin A1c on in-hospital mortality in patients with and without diabetes: findings from the China acute myocardial infarction registry.Cardiovasc Diabetol. 2023 Jul 4;22(1):165. doi: 10.1186/s12933-023-01868-7. Cardiovasc Diabetol. 2023. PMID: 37403082 Free PMC article.
-
Optimal glucose, HbA1c, glucose-HbA1c ratio and stress-hyperglycaemia ratio cut-off values for predicting 1-year mortality in diabetic and non-diabetic acute myocardial infarction patients.Cardiovasc Diabetol. 2021 Oct 19;20(1):211. doi: 10.1186/s12933-021-01395-3. Cardiovasc Diabetol. 2021. PMID: 34666746 Free PMC article.
-
Fasting stress hyperglycemia ratio and in-hospital mortality after acute myocardial infarction in patients with different glucose metabolism status: Results from China acute myocardial infarction registry.Diabetes Res Clin Pract. 2023 Feb;196:110241. doi: 10.1016/j.diabres.2023.110241. Epub 2023 Jan 6. Diabetes Res Clin Pract. 2023. PMID: 36623641
-
Proposal of a New Approach to Study and Categorize Stress Hyperglycemia in Acute Myocardial Infarction.J Emerg Med. 2016 Jul;51(1):31-6. doi: 10.1016/j.jemermed.2015.03.047. Epub 2016 Mar 31. J Emerg Med. 2016. PMID: 27041491 Review.
-
Relationship between stress hyperglycaemic ratio (SHR) and critical illness: a systematic review.Cardiovasc Diabetol. 2025 May 2;24(1):188. doi: 10.1186/s12933-025-02751-3. Cardiovasc Diabetol. 2025. PMID: 40317019 Free PMC article.
Cited by
-
Association between stress hyperglycemia ratio and in-hospital outcomes: findings from the improving Care for Cardiovascular Disease in China-Acute Coronary Syndrome (CCC-ACS) Project.J Geriatr Cardiol. 2024 Jun 28;21(6):658-668. doi: 10.26599/1671-5411.2024.06.006. J Geriatr Cardiol. 2024. PMID: 38973822 Free PMC article.
-
Acute hyperglycemia, a rabble-rouser or innocent bystander? A prospective analysis of clinical implications of acute hyperglycemia in STE-ACS patients.BMC Cardiovasc Disord. 2023 Aug 18;23(1):406. doi: 10.1186/s12872-023-03440-3. BMC Cardiovasc Disord. 2023. PMID: 37596526 Free PMC article. Clinical Trial.
-
Association between admission hyperglycaemia with in-hospital mortality rate in patients with hypertension and acute aortic dissection.J Int Med Res. 2024 Nov;52(11):3000605241291742. doi: 10.1177/03000605241291742. J Int Med Res. 2024. PMID: 39579346 Free PMC article.
-
Glycemic Comparison Index (GCI): a retrospective analysis of its prognostic value in ICU patients with AMI and diabetes.BMC Endocr Disord. 2025 Mar 26;25(1):85. doi: 10.1186/s12902-025-01907-2. BMC Endocr Disord. 2025. PMID: 40140826 Free PMC article.
-
SHRs, biomarkers for dysregulated stress response, predict prognosis in sepsis patients: a retrospective cohort study from MIMIC-IV database.BMC Infect Dis. 2025 Apr 26;25(1):610. doi: 10.1186/s12879-025-11011-4. BMC Infect Dis. 2025. PMID: 40287613 Free PMC article.
References
-
- Qaseem A, Humphrey LL, Chou R, Snow V, Shekelle P. Use of intensive insulin therapy for the management of glycemic control in hospitalized patients: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2011;154:260–267. doi: 10.7326/0003-4819-154-4-201102150-00007. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
